

Application of a framework to guide genetic testing communication across clinical indications
- PMID: 33926532
- PMCID: PMC8086064
- DOI: 10.1186/s13073-021-00887-x
Application of a framework to guide genetic testing communication across clinical indications
Abstract
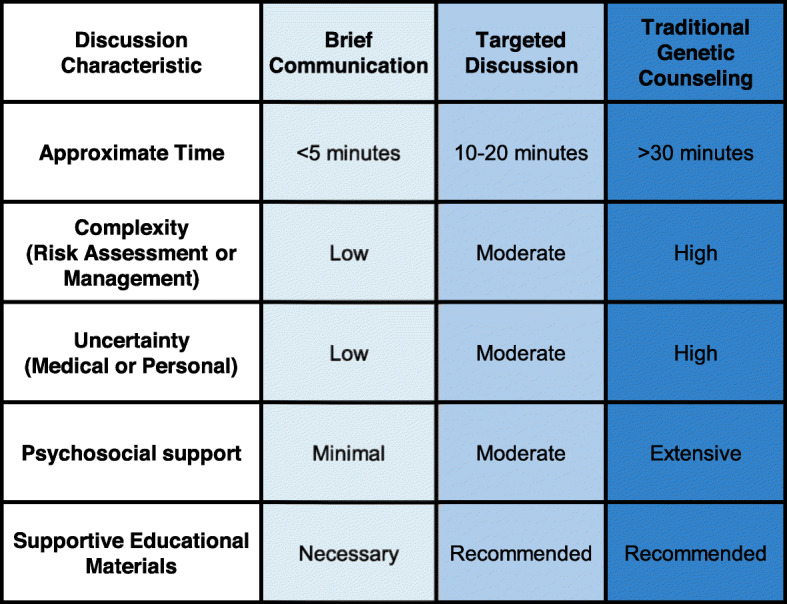
Background: Genetic information is increasingly relevant across healthcare. Traditional genetic counseling (GC) may limit access to genetic information and may be more information and support than some individuals need. We report on the application and clinical implications of a framework to consistently integrate genetics expertise where it is most useful to patients.
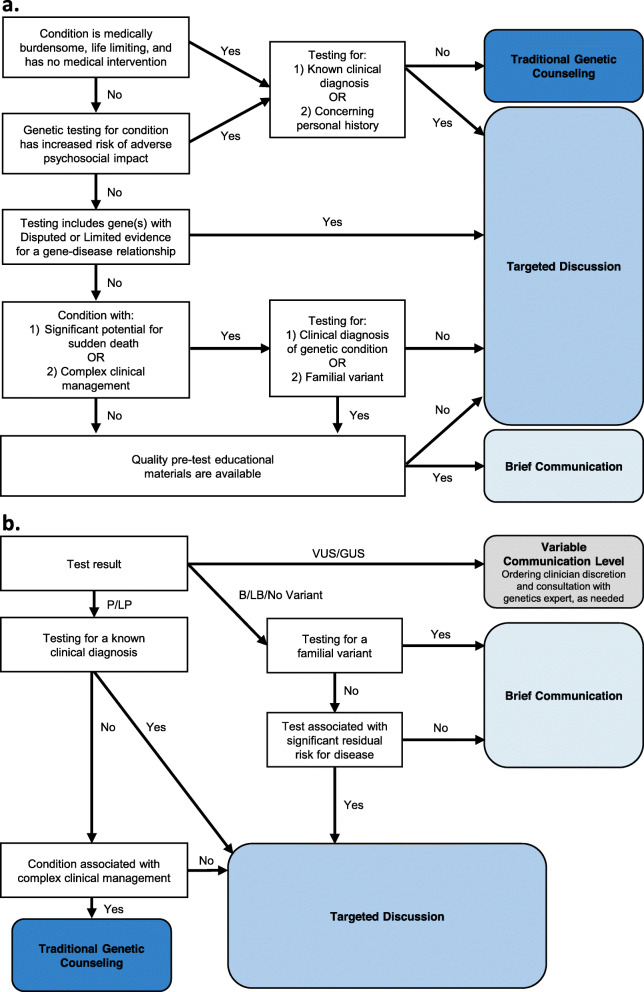
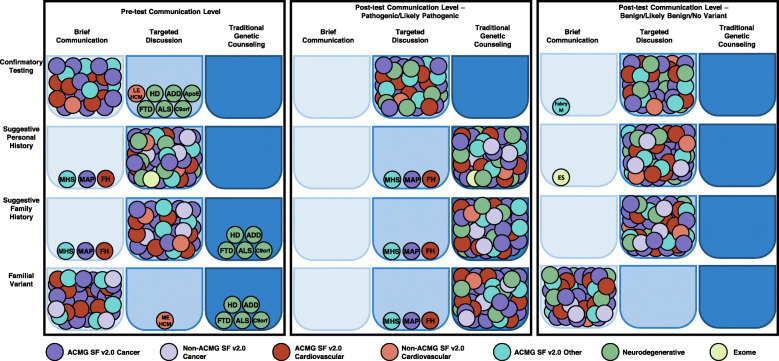
Methods: The Clinical Genome Resource's (ClinGen) Consent and Disclosure Recommendations (CADRe) workgroup designed rubrics to guide pre- and post-genetic test communication. Using a standard set of testing indications, pre- and post-test rubrics were applied to 40 genetic conditions or testing modalities with diverse features, including variability in levels of penetrance, clinical actionability, and evidence supporting a gene-disease relationship. Final communication recommendations were reached by group consensus.
Results: Communication recommendations were determined for 478 unique condition-indication or testing-indication pairs. For half of the conditions and indications (238/478), targeted discussions (moderate communication depth) were the recommended starting communication level for pre- and post-test conversations. Traditional GC was recommended pre-test for adult-onset neurodegenerative conditions for individuals with no personal history and post-test for most conditions when genetic testing revealed a molecular diagnosis as these situations are likely higher in complexity and uncertainty. A brief communication approach was recommended for more straightforward conditions and indications (e.g., familial hypercholesterolemia; familial variant testing).
Conclusions: The CADRe recommendations provide guidance for clinicians in determining the depth of pre- and post-test communication, strategically aligning the anticipated needs of patients with the starting communication approach. Shorter targeted discussions or brief communications are suggested for many tests and indications. Longer traditional GC consultations would be reserved for patients with more complex and uncertain situations where detailed information, education, and psychological support can be most beneficial. Future studies of the CADRe communication framework will be essential for determining if CADRe-informed care supports quality patient experience while improving access to genetic information across healthcare.
Keywords: Access; Genetic counseling; Genetic testing; Informed consent; Results disclosure; Service delivery.
Conflict of interest statement
• AHB has received compensation as a section editor for the
• WRU receives book royalties from Wiley-Blackwell.
• M. Stosic is an employee of DotLab.
• The remaining authors declare that they have no competing interests.
Figures
References
-
- Robson ME, Bradbury AR, Arun B, Domchek SM, Ford JM, Hampel HL, Lipkin SM, Syngal S, Wollins DS, Lindor NM. American Society of Clinical Oncology policy statement update: genetic and genomic testing for cancer susceptibility. J Clin Oncol. 2015;33(31):3660–3667. doi: 10.1200/JCO.2015.63.0996. - DOI - PubMed
-
- MacLeod R, Tibben A, Frontali M, Evers-Kiebooms G, Jones A, Martinez-Descales A, Roos RA, Editorial Committee and Working Group ‘Genetic Testing Counselling’ of the European Huntington Disease Network Recommendations for the predictive genetic test in Huntington’s disease. Clin Genet. 2013;83(3):221–231. doi: 10.1111/j.1399-0004.2012.01900.x. - DOI - PubMed
-
- Riley BD, Culver JO, Skrzynia C, Senter LA, Peters JA, Costalas JW, Callif-Daley F, Grumet SC, Hunt KS, Nagy RS, McKinnon WC, Petrucelli NM, Bennett RL, Trepanier AM. Essential elements of genetic cancer risk assessment, counseling, and testing: updated recommendations of the National Society of Genetic Counselors. J Genet Couns. 2012;21(2):151–161. doi: 10.1007/s10897-011-9462-x. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
