

Higher risk of death from COVID-19 in low-income and non-White populations of São Paulo, Brazil
- PMID: 33926892
- PMCID: PMC8094342
- DOI: 10.1136/bmjgh-2021-004959
Higher risk of death from COVID-19 in low-income and non-White populations of São Paulo, Brazil
Abstract
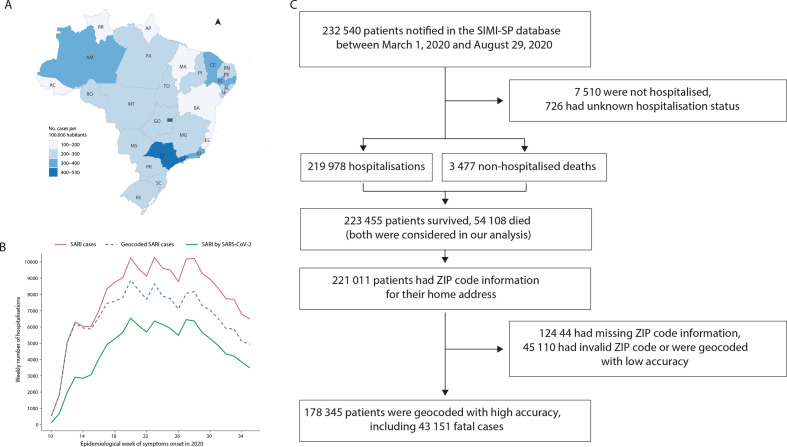
Introduction: Little evidence exists on the differential health effects of COVID-19 on disadvantaged population groups. Here we characterise the differential risk of hospitalisation and death in São Paulo state, Brazil, and show how vulnerability to COVID-19 is shaped by socioeconomic inequalities.
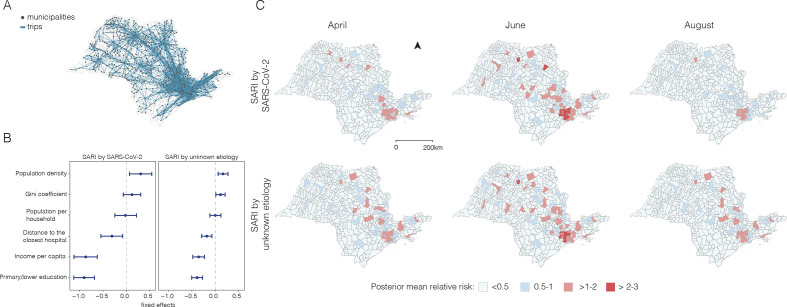
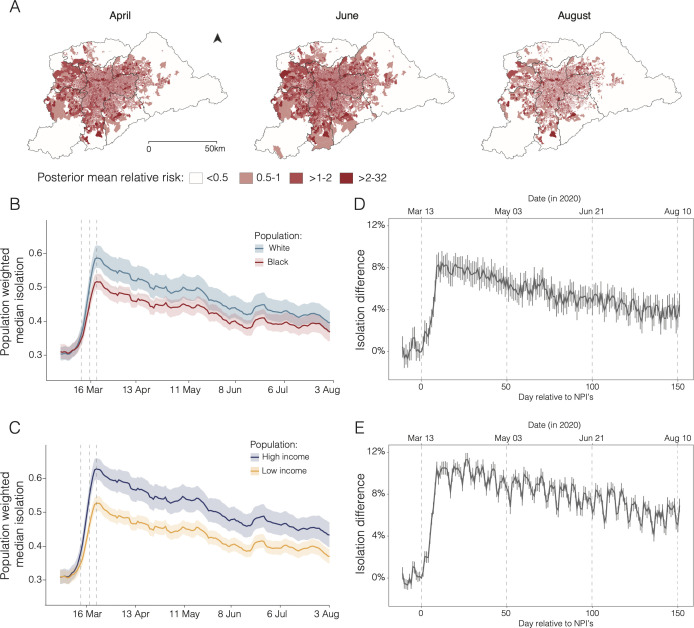
Methods: We conducted a cross-sectional study using hospitalised severe acute respiratory infections notified from March to August 2020 in the Sistema de Monitoramento Inteligente de São Paulo database. We examined the risk of hospitalisation and death by race and socioeconomic status using multiple data sets for individual-level and spatiotemporal analyses. We explained these inequalities according to differences in daily mobility from mobile phone data, teleworking behaviour and comorbidities.
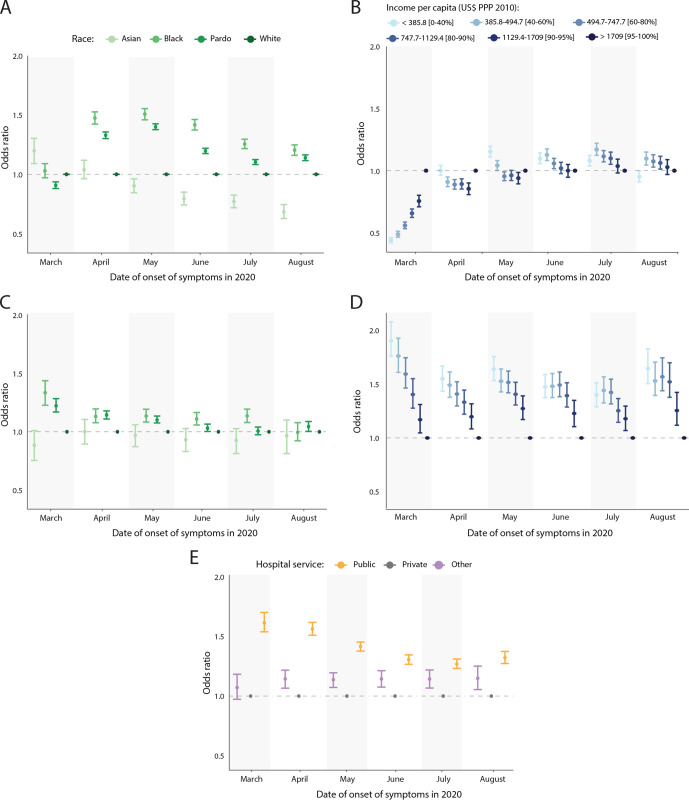
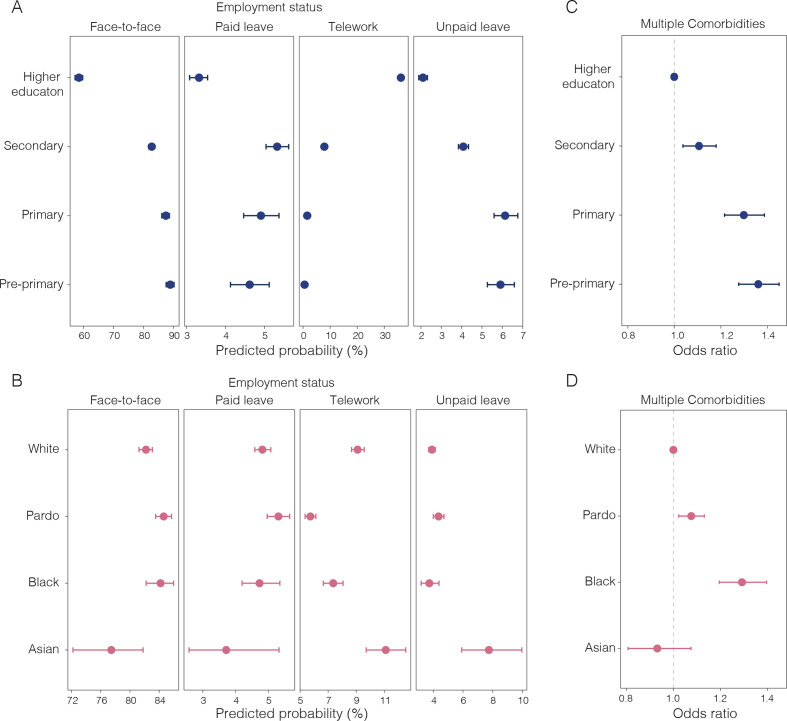
Results: Throughout the study period, patients living in the 40% poorest areas were more likely to die when compared with patients living in the 5% wealthiest areas (OR: 1.60, 95% CI 1.48 to 1.74) and were more likely to be hospitalised between April and July 2020 (OR: 1.08, 95% CI 1.04 to 1.12). Black and Pardo individuals were more likely to be hospitalised when compared with White individuals (OR: 1.41, 95% CI 1.37 to 1.46; OR: 1.26, 95% CI 1.23 to 1.28, respectively), and were more likely to die (OR: 1.13, 95% CI 1.07 to 1.19; 1.07, 95% CI 1.04 to 1.10, respectively) between April and July 2020. Once hospitalised, patients treated in public hospitals were more likely to die than patients in private hospitals (OR: 1.40%, 95% CI 1.34% to 1.46%). Black individuals and those with low education attainment were more likely to have one or more comorbidities, respectively (OR: 1.29, 95% CI 1.19 to 1.39; 1.36, 95% CI 1.27 to 1.45).
Conclusions: Low-income and Black and Pardo communities are more likely to die with COVID-19. This is associated with differential access to quality healthcare, ability to self-isolate and the higher prevalence of comorbidities.
Keywords: cross-sectional survey; epidemiology; geographic information systems; mathematical modelling; public health.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Marmot M, Wilkinson R. Social determinants of health. OUP Oxford, 2005.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous