

Endovascular Treatment of Small and Very Small Intracranial Aneurysms with the Woven EndoBridge Device
- PMID: 33926902
- PMCID: PMC8324278
- DOI: 10.3174/ajnr.A7115
Endovascular Treatment of Small and Very Small Intracranial Aneurysms with the Woven EndoBridge Device
Abstract
Background and purpose: The Woven EndoBridge has proved to be a safe and effective treatment, especially for wide-neck intracranial aneurysms. The recent fifth-generation Woven EndoBridge came with smaller devices. The purpose of this study was to assess the safety and efficiency of Woven EndoBridge treatment of small and very small aneurysms.
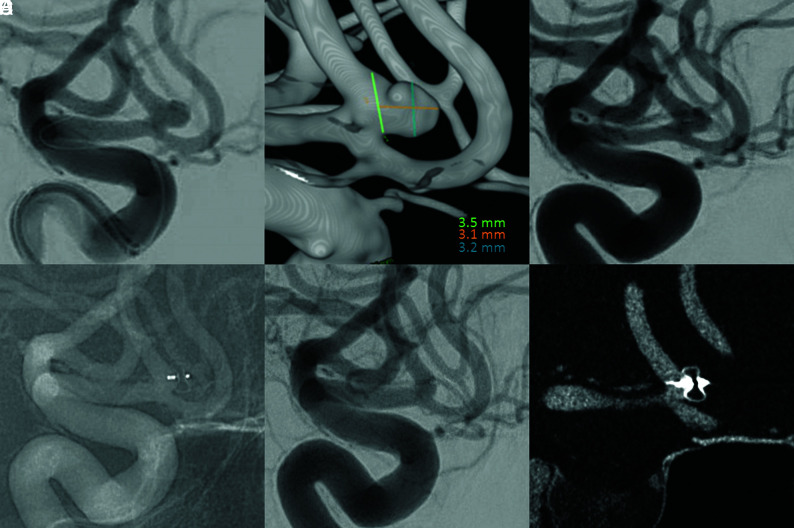
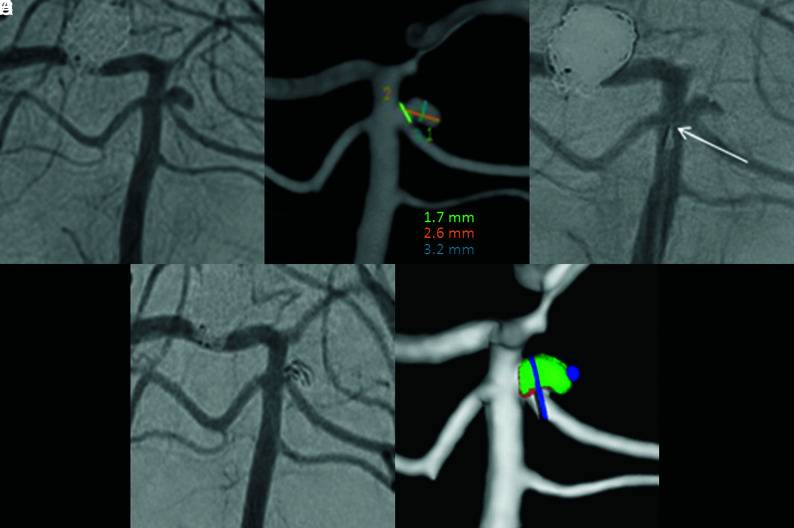
Materials and methods: Between September 2017 and March 2020, all consecutive patients treated with a 3- or 3.5 mm-width Woven EndoBridge device were included in this retrospective intention-to-treat study. Clinical and radiologic findings were evaluated at immediate and last-available follow-up. Angiographic outcome was assessed by an external expert reader.
Results: One hundred twenty-eight aneurysms were treated with a fifth-generation Woven EndoBridge device including 29 with a width of ≤3.5 mm. Ten aneurysms were ruptured (34%). In 3 cases (10%), Woven EndoBridge treatment could not be performed because the aneurysm was still too small for the smallest available Woven EndoBridge device and another endovascular strategy was chosen. The median follow-up time was 11.2 months. Complete and adequate occlusion was obtained in 71% and 90% of the treated aneurysms, respectively. Retreatment was needed in 2 cases (10%). Symptomatic ischemic complications leading to transient neurologic deficits occurred in 2 cases (7%) (1 procedure-related and 1 device-related) but with full spontaneous recovery at discharge.
Conclusions: The fifth-generation Woven EndoBridge device seems to be a safe and technically feasible treatment for both ruptured and unruptured small and very small intracranial aneurysms, with satisfactory occlusion rates on midterm follow-up. However, further study is needed to evaluate longer-term efficiency.
© 2021 by American Journal of Neuroradiology.
Figures
References
-
- Molyneux AJ, Kerr RSC, Yu LM, et al. . International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet 2005;366:809–17 10.1016/S0140-6736(05)67214-5 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical