

FGFR2 Extracellular Domain In-Frame Deletions Are Therapeutically Targetable Genomic Alterations That Function as Oncogenic Drivers in Cholangiocarcinoma
- PMID: 33926920
- PMCID: PMC8690974
- DOI: 10.1158/2159-8290.CD-20-1669
FGFR2 Extracellular Domain In-Frame Deletions Are Therapeutically Targetable Genomic Alterations That Function as Oncogenic Drivers in Cholangiocarcinoma
Abstract
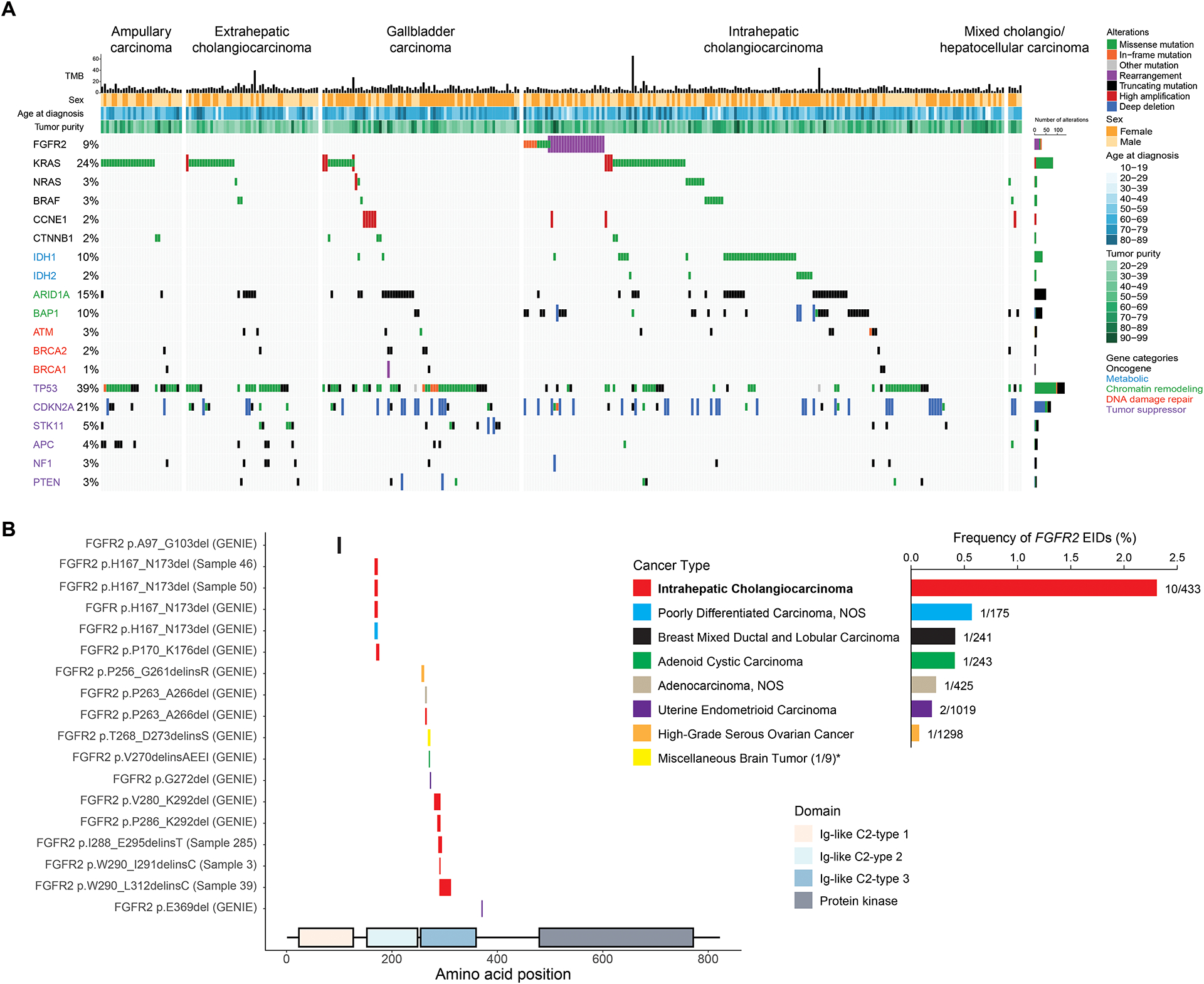
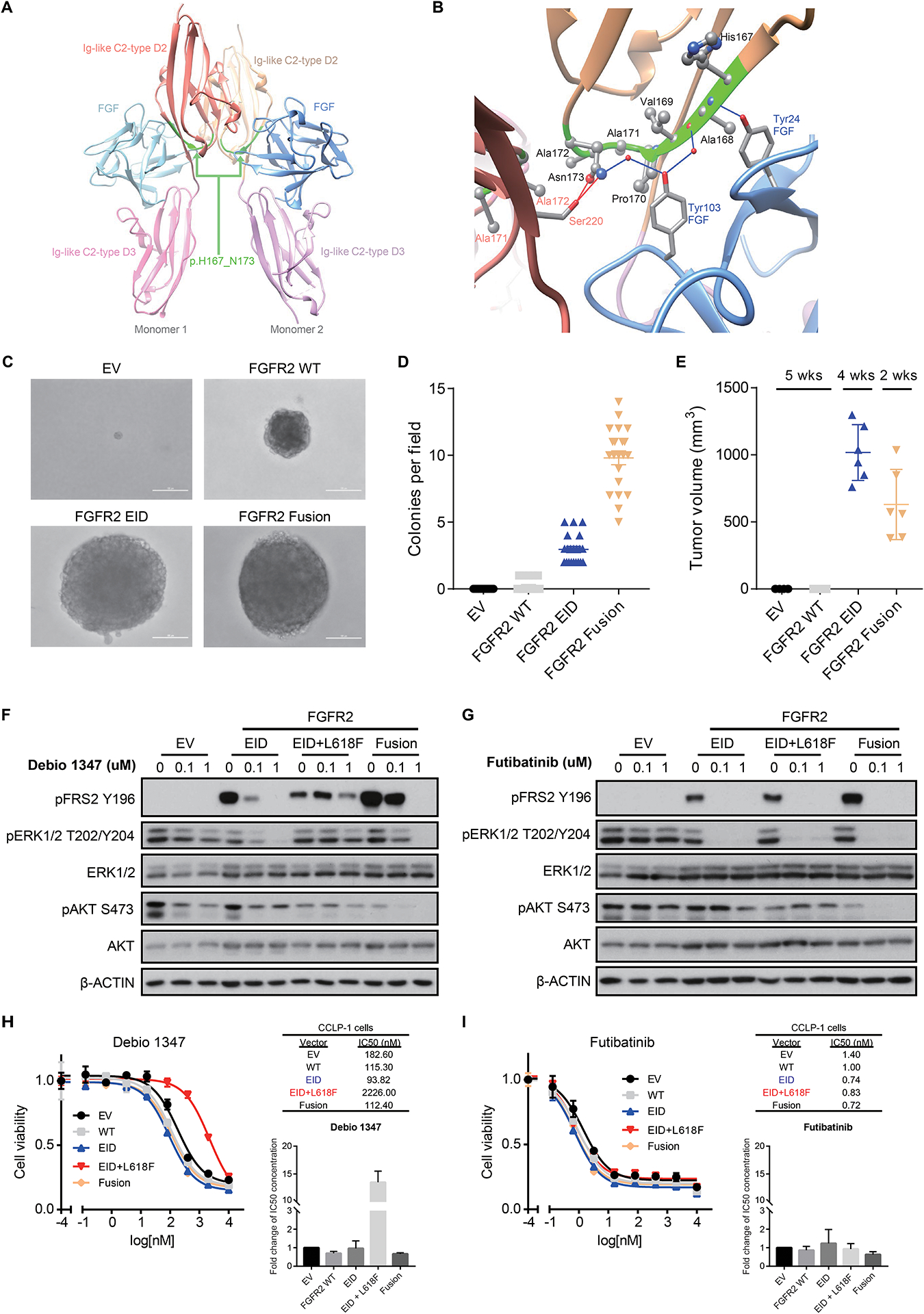
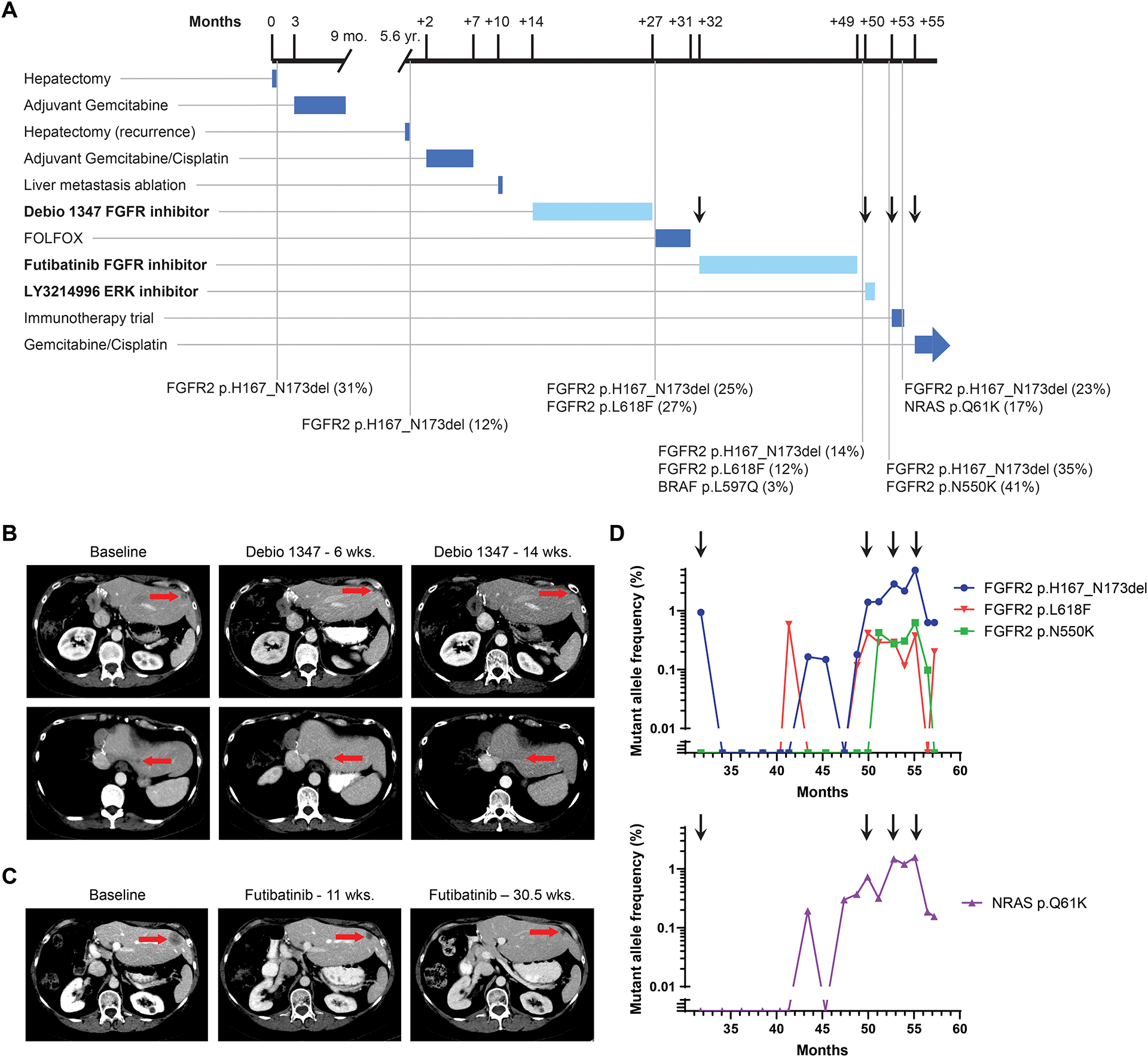
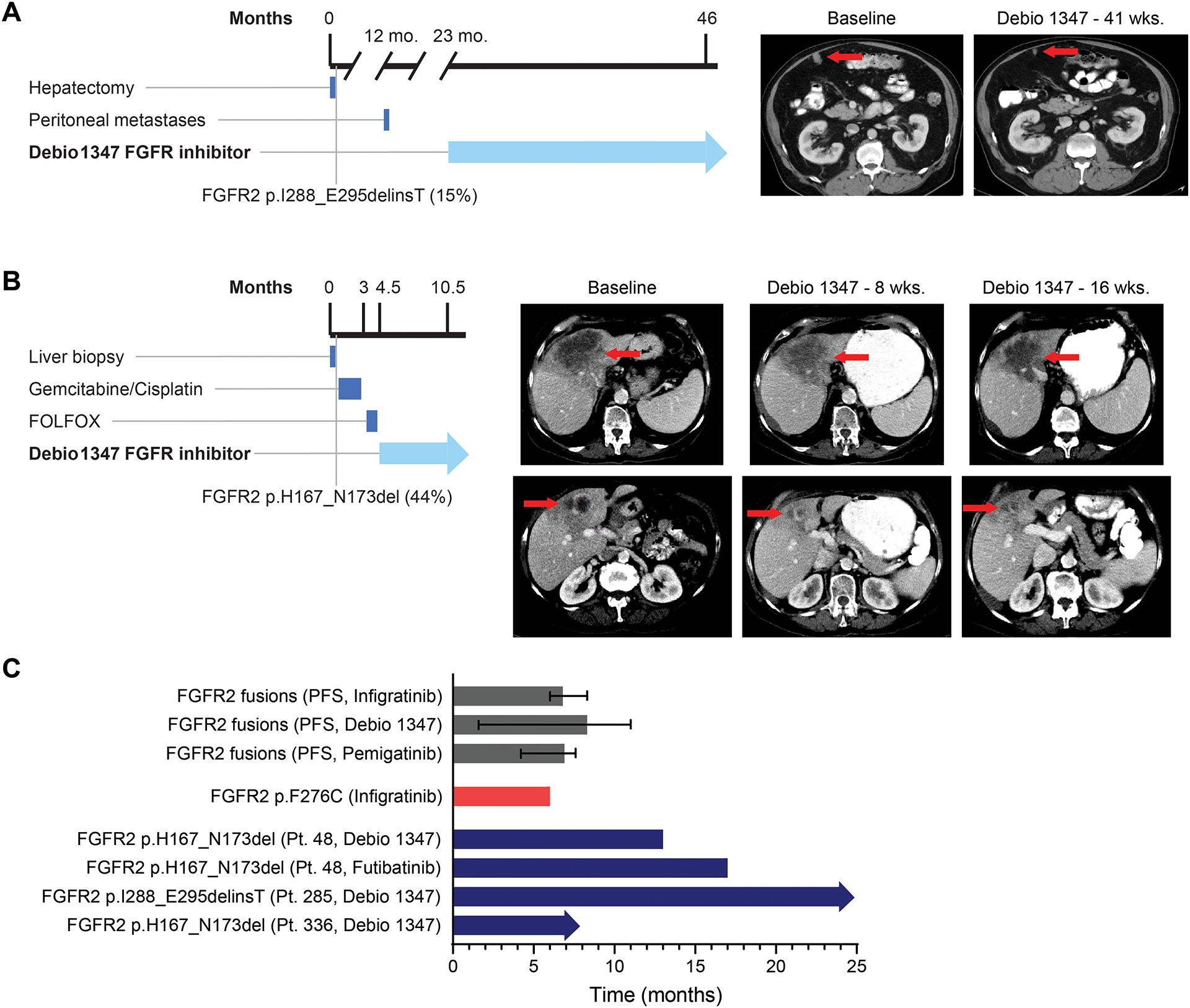
We conducted next-generation DNA sequencing on 335 biliary tract cancers and characterized the genomic landscape by anatomic site within the biliary tree. In addition to frequent FGFR2 fusions among patients with intrahepatic cholangiocarcinoma (IHCC), we identified FGFR2 extracellular domain in-frame deletions (EID) in 5 of 178 (2.8%) patients with IHCC, including two patients with FGFR2 p.H167_N173del. Expression of this FGFR2 EID in NIH3T3 cells resulted in constitutive FGFR2 activation, oncogenic transformation, and sensitivity to FGFR inhibitors. Three patients with FGFR2 EIDs were treated with Debio 1347, an oral FGFR1/2/3 inhibitor, and all showed partial responses. One patient developed an acquired L618F FGFR2 kinase domain mutation at disease progression and experienced a further partial response for 17 months to an irreversible FGFR2 inhibitor, futibatinib. Together, these findings reveal FGFR2 EIDs as an alternative mechanism of FGFR2 activation in IHCC that predicts sensitivity to FGFR inhibitors in the clinic. SIGNIFICANCE: FGFR2 EIDs are transforming genomic alterations that occur predominantly in patients with IHCC. These FGFR2 EIDs are sensitive to FGFR inhibition in vitro, and patients with these alterations benefited from treatment with FGFR inhibitors in the clinic.This article is highlighted in the In This Issue feature, p. 2355.
©2021 American Association for Cancer Research.
Figures
References
-
- Valle JW, Lamarca A, Goyal L, Barriuso J, Zhu AX. New Horizons for Precision Medicine in Biliary Tract Cancers. Cancer Discov 2017;7(9):943–62 doi 10.1158/2159-8290.Cd-17-0245. - DOI - PMC - PubMed
-
- Goyal L, Shi L, Liu LY, Fece de la Cruz F, Lennerz JK, Raghavan S, et al. TAS-120 Overcomes Resistance to ATP-Competitive FGFR Inhibitors in Patients with FGFR2 Fusion-Positive Intrahepatic Cholangiocarcinoma. Cancer Discov 2019;9(8):1064–79 doi 10.1158/2159-8290.CD-19-0182. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
