

Viability and thresholds for treatment of extremely preterm infants: survey of UK neonatal professionals
- PMID: 33927001
- PMCID: PMC8543207
- DOI: 10.1136/archdischild-2020-321273
Viability and thresholds for treatment of extremely preterm infants: survey of UK neonatal professionals
Abstract
Background: Decisions about treatments for extremely preterm infants (EPIs) born in the 'grey zone' of viability can be ethically complex. This 2020 survey aimed to determine views of UK neonatal staff about thresholds for treatment of EPIs given a recently revised national Framework for Practice from the British Association of Perinatal Medicine.
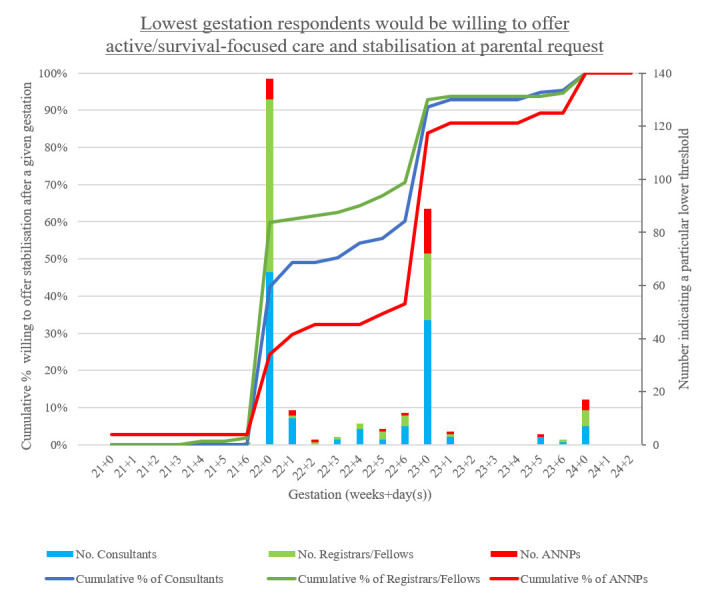
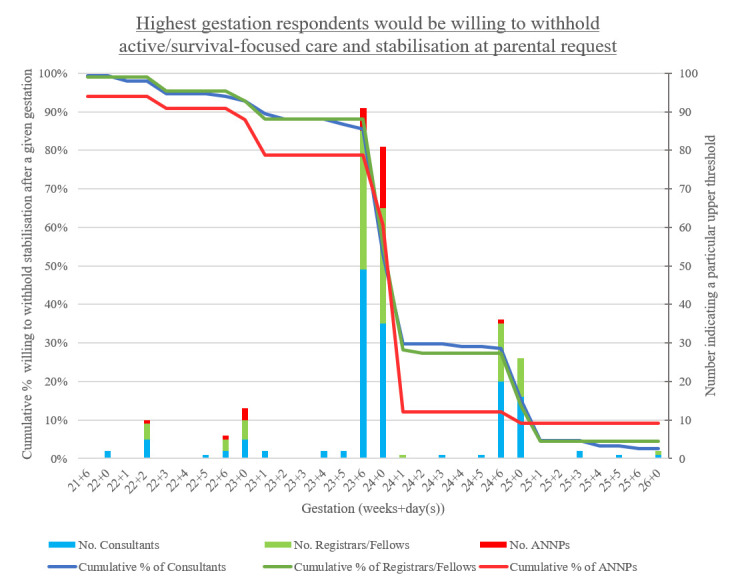
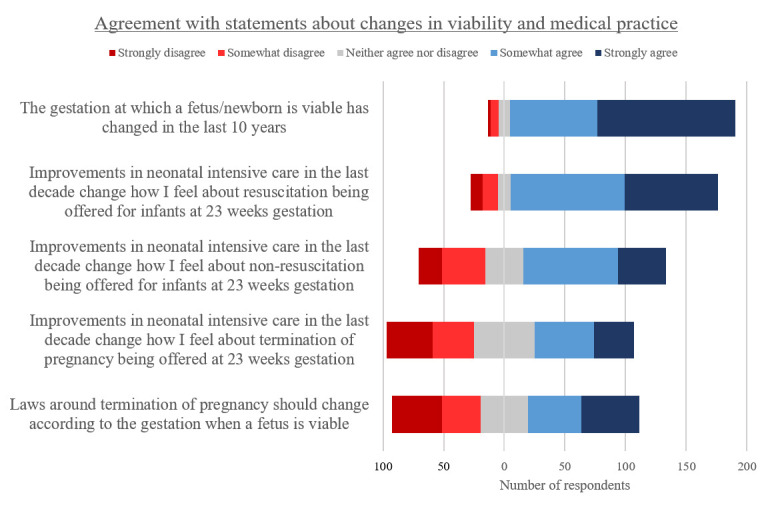
Methods: The online survey requested participants indicate the lowest gestation at which they would be willing to offer active treatment and the highest gestation at which they would withhold active treatment of an EPI at parental request (their lower and upper thresholds). Relative risks were used to compare respondents' views based on profession and neonatal unit designation. Further questions explored respondents' conceptual understanding of viability.
Results: 336 respondents included 167 consultants, 127 registrars/fellows and 42 advanced neonatal nurse practitioners (ANNPs). Respondents reported a median grey zone for neonatal resuscitation between 22+1 and 24+0 weeks' gestation. Registrars/fellows were more likely to select a lower threshold at 22+0 weeks compared with consultants (Relative Risk (RR)=1.37 (95% CI 1.07 to 1.74)) and ANNPs (RR=2.68 (95% CI 1.42 to 5.06)). Those working in neonatal intensive care units compared with other units were also more likely to offer active treatment at 22+0 weeks (RR=1.86 (95% CI 1.18 to 2.94)). Most participants understood a fetus/newborn to be 'viable' if it was possible to survive, regardless of disability, with medical interventions accessible to the treating team.
Conclusion: Compared with previous studies, we found a shift in the reported lower threshold for resuscitation in the UK, with greater acceptance of active treatment for infants <23 weeks' gestation.
Keywords: ethics; neonatology; palliative care; resuscitation.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: DW, HM and SEB were part of British Association of Perinatal Medicine working group that developed the 2019 Framework for Practice.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical