

Pulmonary fibrosis 4 months after COVID-19 is associated with severity of illness and blood leucocyte telomere length
- PMID: 33927016
- PMCID: PMC8103561
- DOI: 10.1136/thoraxjnl-2021-217031
Pulmonary fibrosis 4 months after COVID-19 is associated with severity of illness and blood leucocyte telomere length
Abstract
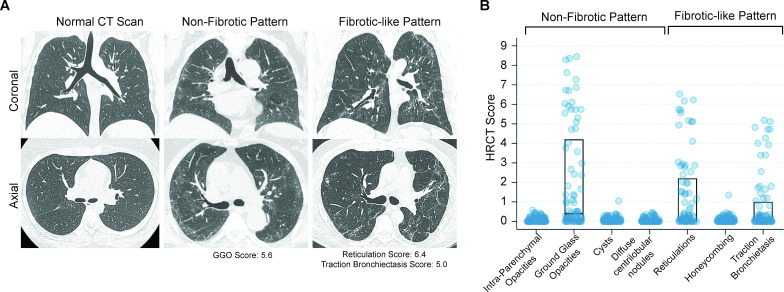
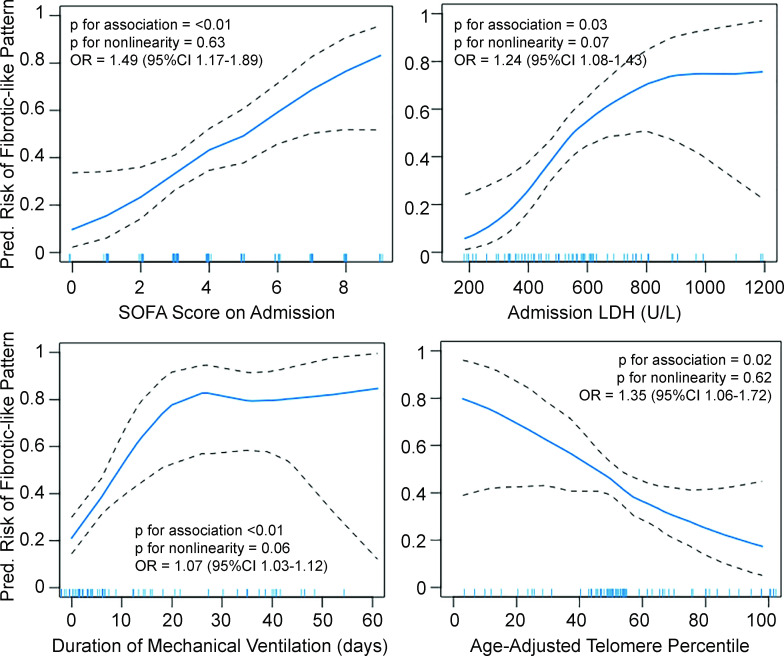
The risk factors for development of fibrotic-like radiographic abnormalities after severe COVID-19 are incompletely described and the extent to which CT findings correlate with symptoms and physical function after hospitalisation remains unclear. At 4 months after hospitalisation, fibrotic-like patterns were more common in those who underwent mechanical ventilation (72%) than in those who did not (20%). We demonstrate that severity of initial illness, duration of mechanical ventilation, lactate dehydrogenase on admission and leucocyte telomere length are independent risk factors for fibrotic-like radiographic abnormalities. These fibrotic-like changes correlate with lung function, cough and measures of frailty, but not with dyspnoea.
Keywords: COVID-19; imaging/CT MRI etc; interstitial fibrosis; respiratory measurement; viral infection.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical