

Relationship between heart failure and the risk of acute exacerbation of COPD
- PMID: 33927022
- PMCID: PMC8311079
- DOI: 10.1136/thoraxjnl-2020-216390
Relationship between heart failure and the risk of acute exacerbation of COPD
Abstract
Rationale: Heart failure (HF) management in chronic obstructive pulmonary disease (COPD) is often delayed or suboptimal.
Objectives: To examine the effect of HF and HF medication use on moderate-to-severe COPD exacerbations.
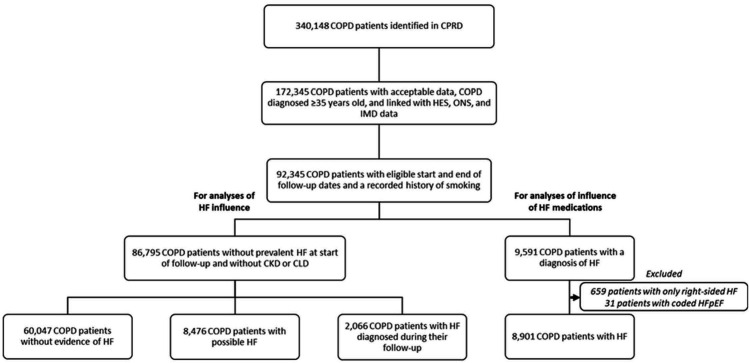
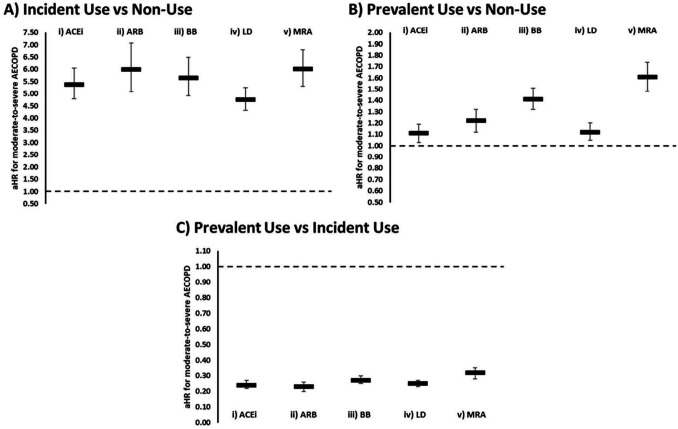
Methods and measurements: Retrospective cohort studies from 2006 to 2016 using nationally representative English primary care electronic healthcare records linked to national hospital and mortality data. Patients with COPD with diagnosed and possible HF were identified. Possible HF was defined as continuous loop diuretic use in the absence of a non-cardiac indication. Incident exposure to HF medications was defined as ≥2 prescriptions within 90 days with no gaps >90 days during ≤6 months of continuous use; prevalent exposure as 6+ months of continuous use. HF medications investigated were angiotensin receptor blockers, ACE inhibitors, beta-blockers, loop diuretics and mineralocorticoid receptor antagonists. Cox regression, stratified by sex and age, further adjusted for patient characteristics, was used to determine the association of HF with exacerbation risk.
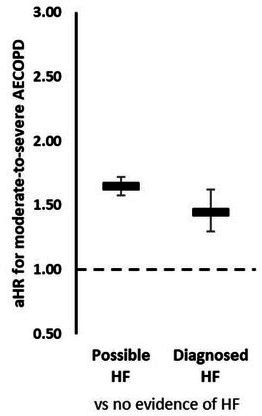
Main results: 86 795 patients with COPD were categorised as no evidence of HF (n=60 047), possible HF (n=8476) and newly diagnosed HF (n=2066). Newly diagnosed HF (adjusted HR (aHR): 1.45, 95% CI: 1.30 to 1.62) and possible HF (aHR: 1.65, 95% CI: 1.58 to 1.72) similarly increased exacerbation risk. Incident and prevalent use of all HF medications were associated with increased exacerbation risk. Prevalent use was associated with reduced exacerbation risk compared with incident use.
Conclusions: Earlier opportunities to improve the diagnosis and management of HF in the COPD population are missed. Managing HF may reduce exacerbation risk in the long term.
Keywords: COPD epidemiology; COPD exacerbations; clinical epidemiology.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: ELA has nothing to disclose. AB reports grants from Dr Foster, during the conduct of the study, and grants from Medtronic, outside the submitted work. MRC reports receiving research funding and speaker fees from ResMed, Boston Scientific, Medtronic and Abbott, and consultancy and speaker fees from Servier, Novartis, Vifor, LivaNova, Pfizer, Roche Diagnostics and Amgen, outside the submitted work. JKQ reports grants from MRC, grants from BLF, grants from The Health Foundation, grants and personal fees from AZ, grants and personal fees from BI, grants from Chiesi, grants and personal fees from Bayer, and grants and personal fees from GSK, outside the submitted work.
Figures
References
-
- GOLD . Global strategy for the diagnosis, management and prevention of COPD, global initiative for chronic obstructive lung disease (GOLD) 2017 [Webpage], 2017. Available: http://goldcopd.org/gold-2017-global-strategy-diagnosis-management-preve... [Accessed 10 Jan 2018].
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators . Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet 2018;392:1789–858. 10.1016/S0140-6736(18)32279-7 - DOI - PMC - PubMed
-
- Rutten FH. Diagnosis and mangement of heart failure in COPD. In: Rabe KF, Wedzicha JA, Wouters EF, eds. Eur respir monogr, 2013: 50–63.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous