Magnetic Resonance Imaging in Peripartum Encephalopathy: A Pictorial Review
- PMID: 33927531
- PMCID: PMC8064849
- DOI: 10.1055/s-0041-1727300
Magnetic Resonance Imaging in Peripartum Encephalopathy: A Pictorial Review
Abstract
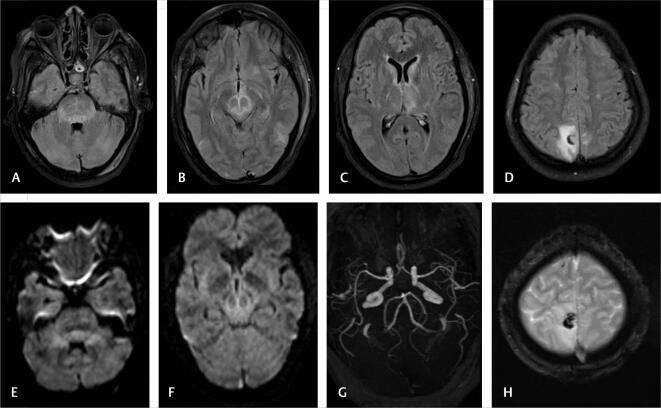
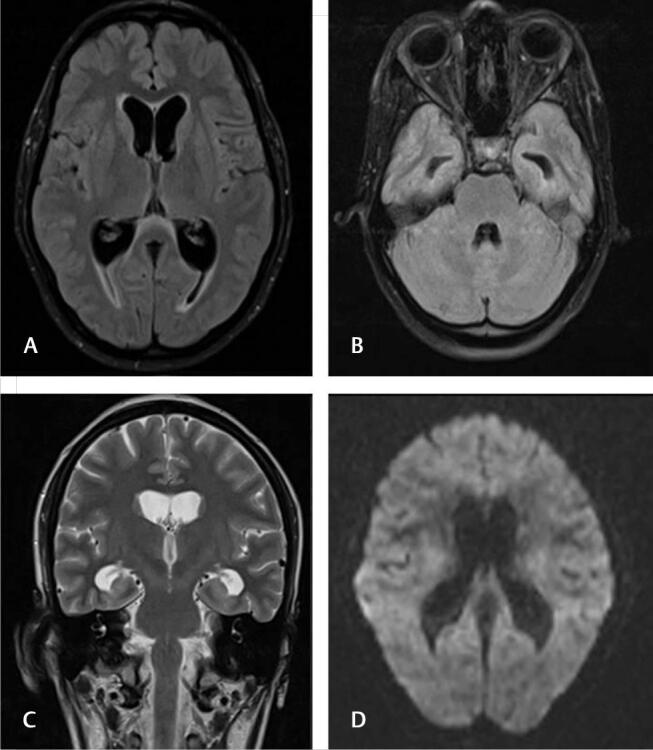
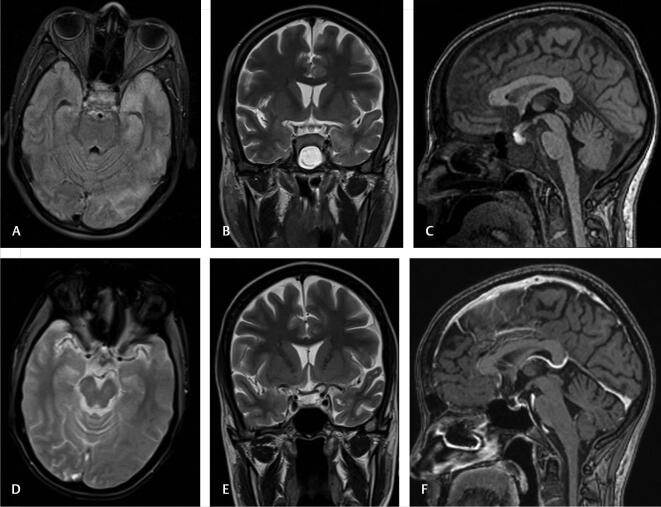
Acute neurological problems are significant disorders of pre- and postpartum period in women. We analyzed the magnetic resonance imaging (MRI) profile of patients presenting with peripartum encephalopathy over 2 years. Of 51 patients, MRI was abnormal in 40 patients and normal in 11 patients. Posterior reversible encephalopathy (13/40), cerebral venous thrombosis (6/40), and postpartum angiopathy (3/40) are the three most common causes of peripartum encephalopathy as identified in MRI. The other less common but important etiology include HELLP (Hemolysis, Elevated Liver enzymes and Low Platelet) syndrome (2), osmotic demyelination (2), antiphospholipid syndrome (2), tubercular meningitis/cerebritis (3), pituitary hyperplasia with hemorrhage (2), postictal edema (2), cerebellitis (1), transient splenial lesion (1), and changes of old trauma and stroke (one each).
Keywords: magnetic resonance imaging; peripartum encephalopathy; posterior reversible encephalopathy; postpartum angiopathy.
Association for Helping Neurosurgical Sick People. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Conflict of Interest None declared.
Figures










References
-
- Lamy C, Sharshar T, Mas J L. [Cerebrovascular diseases in pregnancy and puerperium] Rev Neurol (Paris) 1996;152(06/07):422–440. - PubMed
-
- Dineen R, Banks A, Lenthall R. Imaging of acute neurological conditions in pregnancy and the puerperium. Clin Radiol. 2005;60(11):1156–1170. - PubMed
-
- Al-Hayali R M, Al-Habbo D J, Hammo M K. Peripartum neurological emergencies in a critical care unit. Neurosciences (Riyadh) 2008;13(02):155–160. - PubMed