

Unique Profile of Driver Gene Mutations in Patients With Non-Small-Cell Lung Cancer in Qujing City, Yunnan Province, Southwest China
- PMID: 33928034
- PMCID: PMC8076749
- DOI: 10.3389/fonc.2021.644895
Unique Profile of Driver Gene Mutations in Patients With Non-Small-Cell Lung Cancer in Qujing City, Yunnan Province, Southwest China
Abstract
Objective: Qujing City, Yunnan Province, China, has a high incidence of lung cancer and related mortality. The etiology of NSCLC in Qujing area and distribution of associated molecular aberrations has not been fully elucidated. This study aimed to reveal the profile of driver gene mutations in patients with non-small-cell lung cancer (NSCLC) in Qujing and explore their relationships with clinicopathological characteristics.
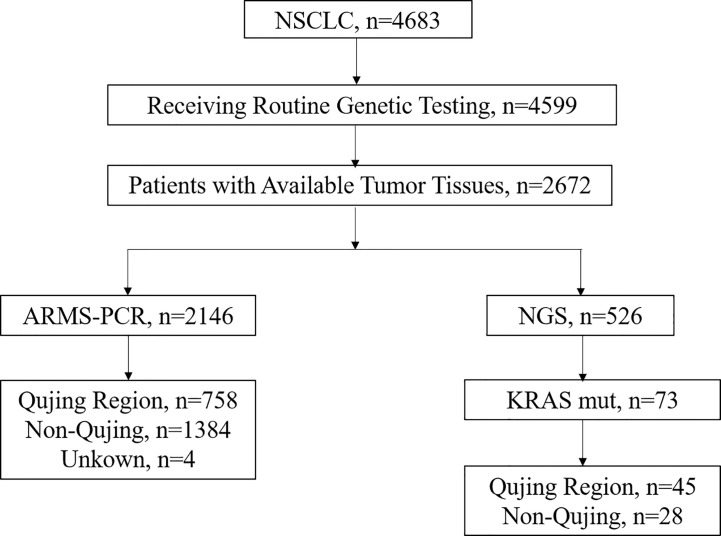
Methods: In this study, the mutation profiles of NSCLC driver genes, including EGFR, ALK, ROS1, KRAS, BRAF, RET, MET, HER2, NRAS, and PIK3CA, were investigated in patients with NSCLC from Qujing and compared with those from other regions in Yunnan Province. The associations between molecular mutations and clinicopathological characteristics were further analyzed.
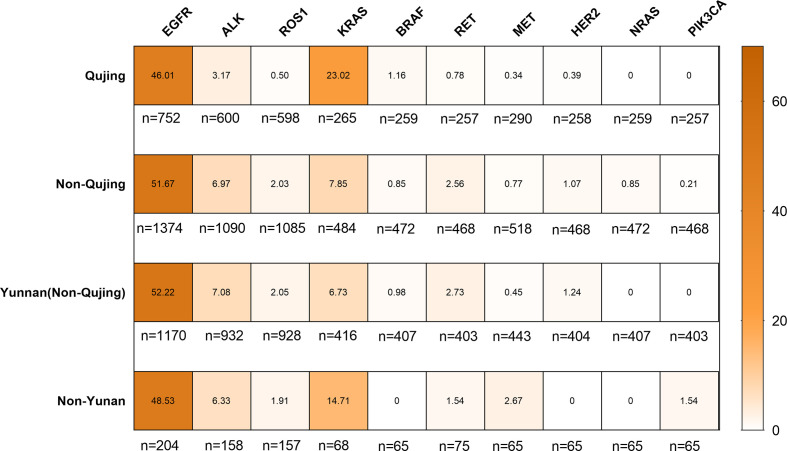
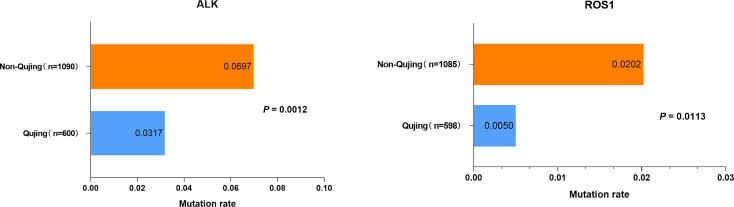
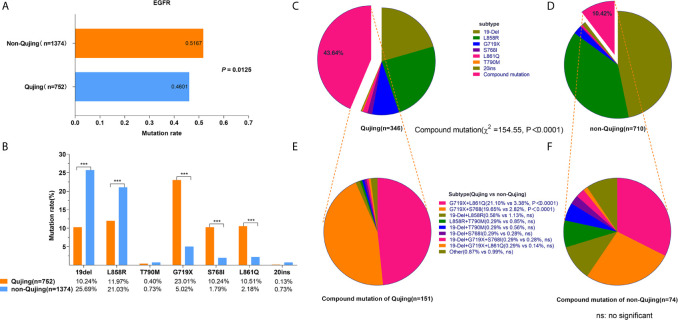
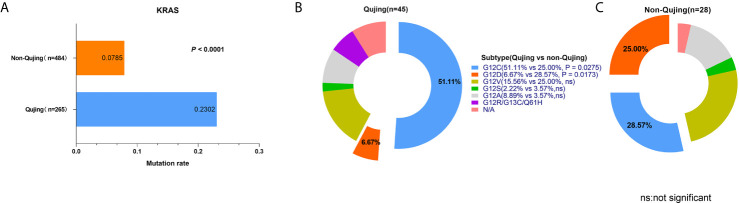
Results: A distinct profile of driver gene mutations was discovered in patients with NSCLC from Qujing. Interestingly, a higher proportion of EGFR compound mutations, including G719X + S768I (19.65% vs 3.38%, P < 0.0001) and G719X + L861Q (21.10% vs 2.82%, P < 0.0001), was observed in patients with NSCLC in Qujing compared with patients in non-Qujing area, besides significantly different distributions of EGFR (46.01% vs. 51.07%, P = 0.0125), ALK (3.17% vs. 6.97%, P = 0.0012), ROS1 (0.5% vs. 2.02%, P = 0.0113), and KRAS (23.02% vs. 7.85%, P < 0.0001). Further, EGFR compound mutations were more likely associated with the occupation of patients (living/working in rural areas, e.g., farmers). Moreover, KRAS G12C was the dominant subtype (51.11% vs 25.00%, P = 0.0275) among patients with NSCLC having KRAS mutations in Qujing.
Conclusions: Patients with NSCLC in Qujing displayed a unique profile of driver gene mutations, especially a higher prevalence of EGFR compound mutations and dominant KRAS G12C subtype, in this study, indicating a peculiar etiology of NSCLC in Qujing. Therefore, a different paradigm of therapeutic strategy might need to be considered for patients with NSCLC in Qujing.
Keywords: ALK; EGFR; KRAS; Qujing; ROS1; mutation profile; non-small-cell lung cancer.
Copyright © 2021 Zhou, Ge, Du, Li, Cai, Liu, Guo, Shen, Duan, Huang, Yao, Zhu, Shi and Huang.
Conflict of interest statement
ZH, FY, and CZ were employed by Amoy Diagnostics Co., Ltd. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous