

Development of an automated ERCP Quality Report Card using structured data fields
- PMID: 33928265
- PMCID: PMC8078858
- DOI: 10.1016/j.tige.2021.01.005
Development of an automated ERCP Quality Report Card using structured data fields
Abstract
Background and aims: Measuring adherence to ERCP quality indicators (QIs) is confounded by variability in indications, maneuvers, and documentation styles. We hypothesized that incorporation of mandatory, structured data fields within reporting software would permit accurate measurement of QI adherence rates and facilitate generation of a provider ERCP report card.
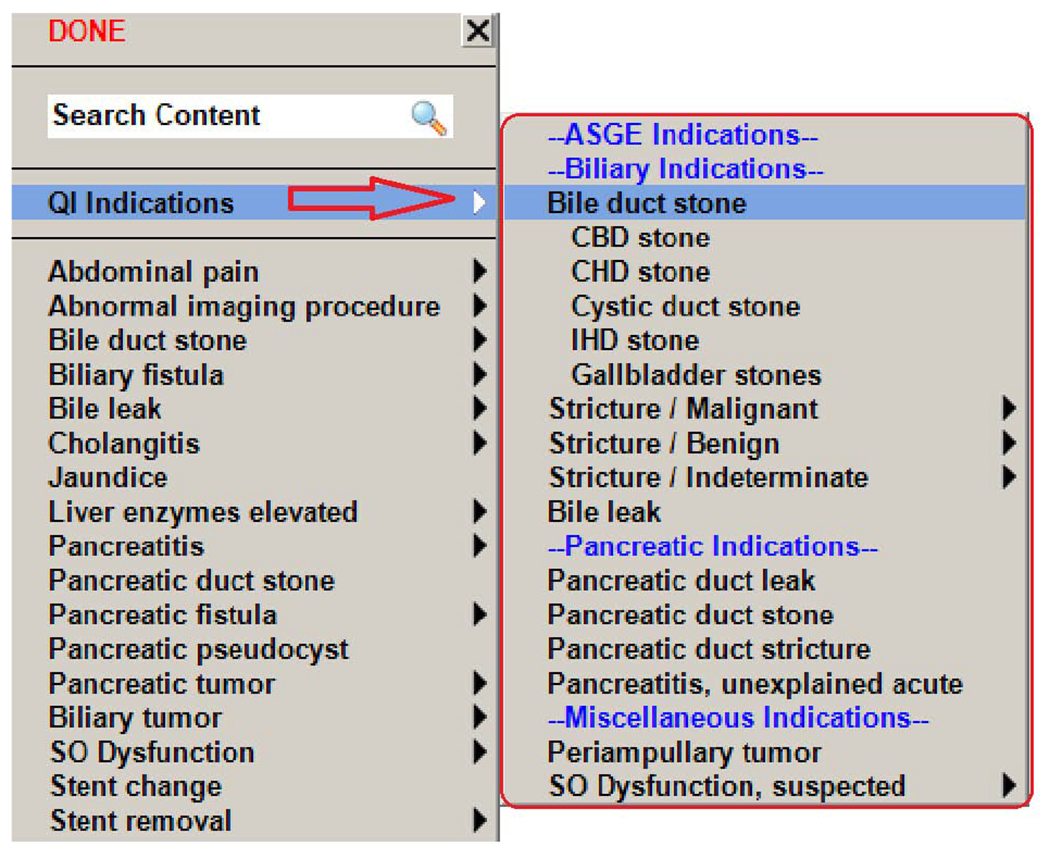
Methods: At two referral centers, endoscopy documentation software was modified to generate provider alerts prior to finalizing the note. The alerts reminded the provider to document the following components in a standardized manner: indication, altered anatomy, prior interventions, and QIs deemed high priority by society consensus, study authors, or both. Adherence rates for each QI were calculated in aggregate and by provider via data extraction directly from the procedure documentation software. Medical records were reviewed manually to measure the accuracy of automated data extraction. Accuracy of automated measurement for each QI was calculated against results derived by manual review.
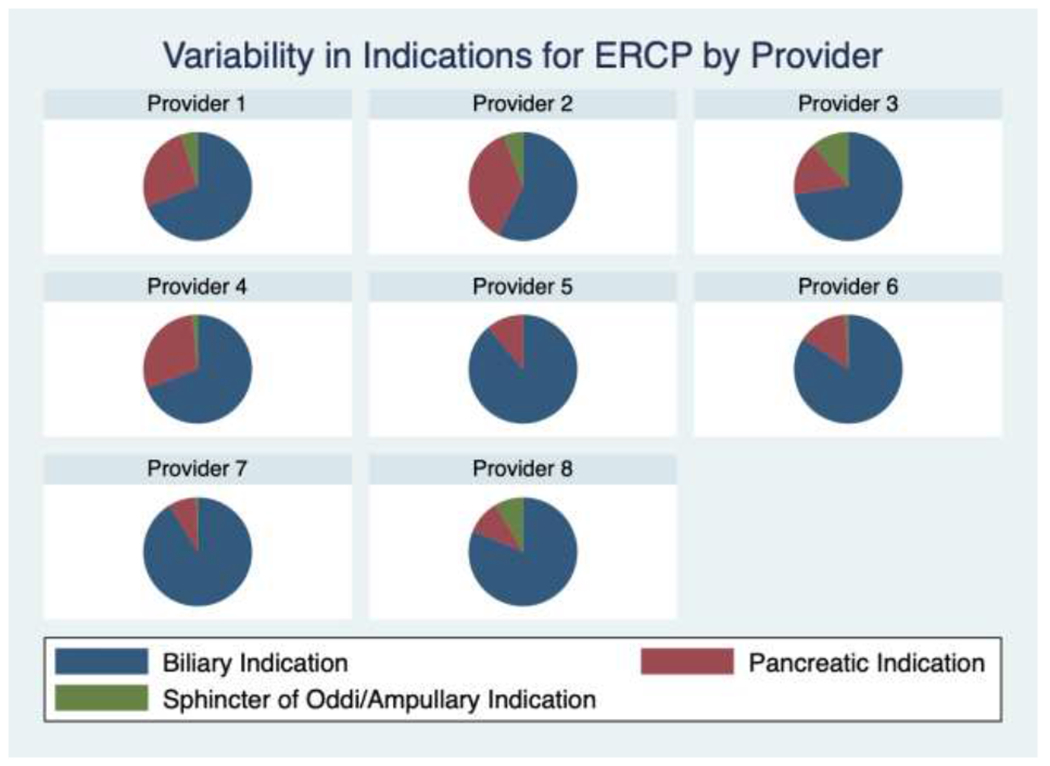
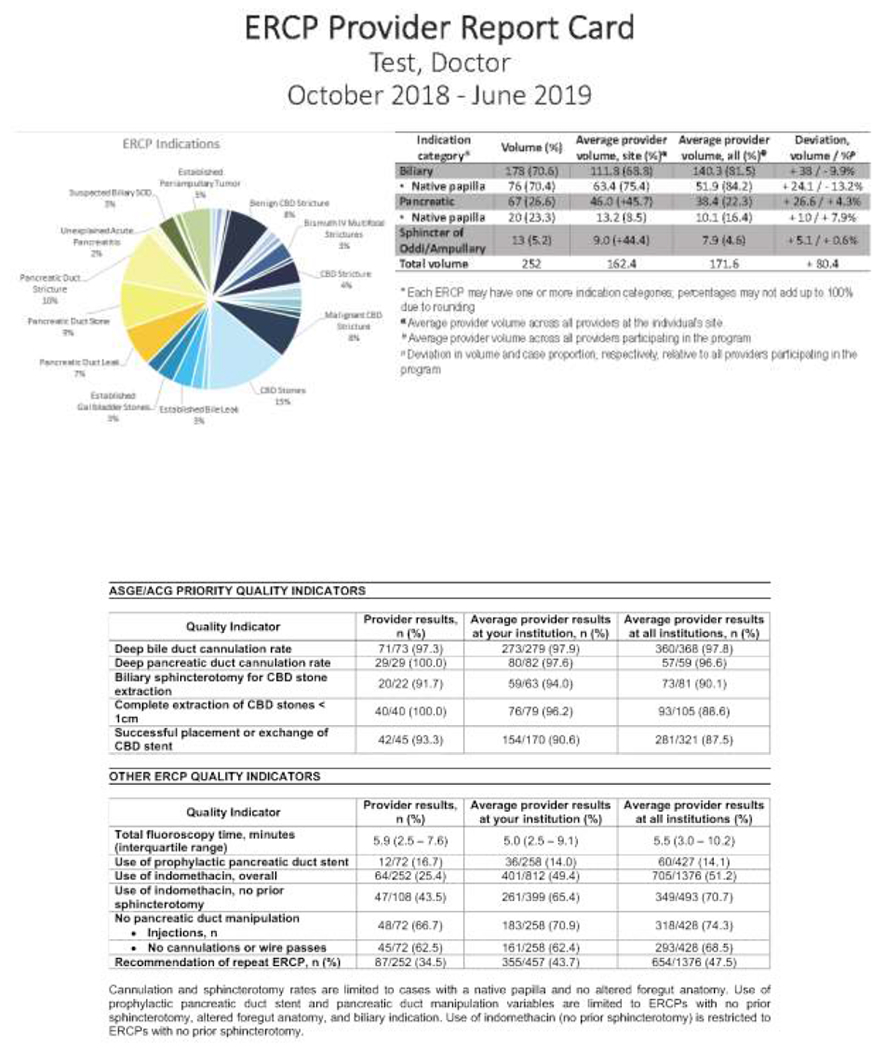
Results: During the 9-month study period, 1,376 ERCP procedures were completed by 8 providers. Manual medical record review confirmed high (98-100%) accuracy of automatic extraction of ERCP QIs from the endoscopy report, including cannulation rate of the native papilla and complete extraction of common bile duct stones. An ERCP report card was generated, allowing for individual comparison of adherence to ERCP QIs with colleagues at their institution and others.
Conclusion: In this pilot study, use of mandatory, structured data fields within clinical ERCP reports permit the accurate measurement of high priority ERCP QIs and the subsequent generation of interval report cards.
Keywords: Benchmarking; Cholangiopancreatography; Electronic Health Records; Endoscopic Retrograde; Health Care; Quality Indicators.
Conflict of interest statement
Potential competing interests: Michael McMurtry is an employee of Provation Medical. All other authors (Gregory Cote, B. Joseph Elmunzer, Erin Forster, Robert Moran, John Quiles, Daniel Strand, Dushant Uppal, Andrew Wang, Peter Cotton, and James Scheiman) report no financial relationships with a commercial entity producing health-care related products and/or services relevant to this article.
Figures
Similar articles
-
Quality Indicators of Endoscopic Retrograde Cholangiopancreatography in Korea.Gut Liver. 2024 Jul 15;18(4):564-577. doi: 10.5009/gnl230427. Epub 2024 Mar 11. Gut Liver. 2024. PMID: 38462478 Free PMC article. Review.
-
Papillary cannulation and sphincterotomy techniques at ERCP: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline.Endoscopy. 2016 Jul;48(7):657-83. doi: 10.1055/s-0042-108641. Epub 2016 Jun 14. Endoscopy. 2016. PMID: 27299638
-
'Short' double-balloon enteroscope endoscopic retrograde cholangiopancreatography in patients with a surgically altered upper gastrointestinal tract.Can J Gastroenterol. 2011 Nov;25(11):615-9. doi: 10.1155/2011/354546. Can J Gastroenterol. 2011. PMID: 22059169 Free PMC article.
-
Surgeon-performed endoscopic retrograde cholangiopancreatography. Outcomes of 2392 procedures at two tertiary care centers.Surg Endosc. 2018 Jun;32(6):2871-2876. doi: 10.1007/s00464-017-5995-x. Epub 2017 Dec 22. Surg Endosc. 2018. PMID: 29273876 Free PMC article.
-
Performance measures for endoscopic retrograde cholangiopancreatography and endoscopic ultrasound: A European Society of Gastrointestinal Endoscopy (ESGE) Quality Improvement Initiative.United European Gastroenterol J. 2018 Dec;6(10):1448-1460. doi: 10.1177/2050640618808157. Epub 2018 Oct 19. United European Gastroenterol J. 2018. PMID: 30574315 Free PMC article. Review.
References
-
- Cotton PB, Feussner D, Dufault D, et al. A survey of credentialing for ERCP in the United States. Gastrointest Endosc 2017;86:866–869. - PubMed
-
- Cotton PB, Romagnuolo J, Faigel DO, et al. The ERCP quality network: a pilot study of benchmarking practice and performance. Am J Med Qual 2013;28:256–60. - PubMed
-
- Calderwood AH, Holub JL , Greenwald DA, et al. Yield and Practice Patterns of Surveillance Colonoscopy Among Older Adults: An Analysis of the GI Quality Improvement Consortium. Am J Gastroenterol 2019;114:1811–1819. - PubMed
-
- Kaminski MF, Wieszczy P, Rupinski M, et al. Increased Rate of Adenoma Detection Associates With Reduced Risk of Colorectal Cancer and Death. Gastroenterology 2017;153:98–105. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources