

Clinical features of migraine with onset prior to or during start of combined hormonal contraception: a prospective cohort study
- PMID: 33928470
- PMCID: PMC8986701
- DOI: 10.1007/s13760-021-01677-3
Clinical features of migraine with onset prior to or during start of combined hormonal contraception: a prospective cohort study
Abstract
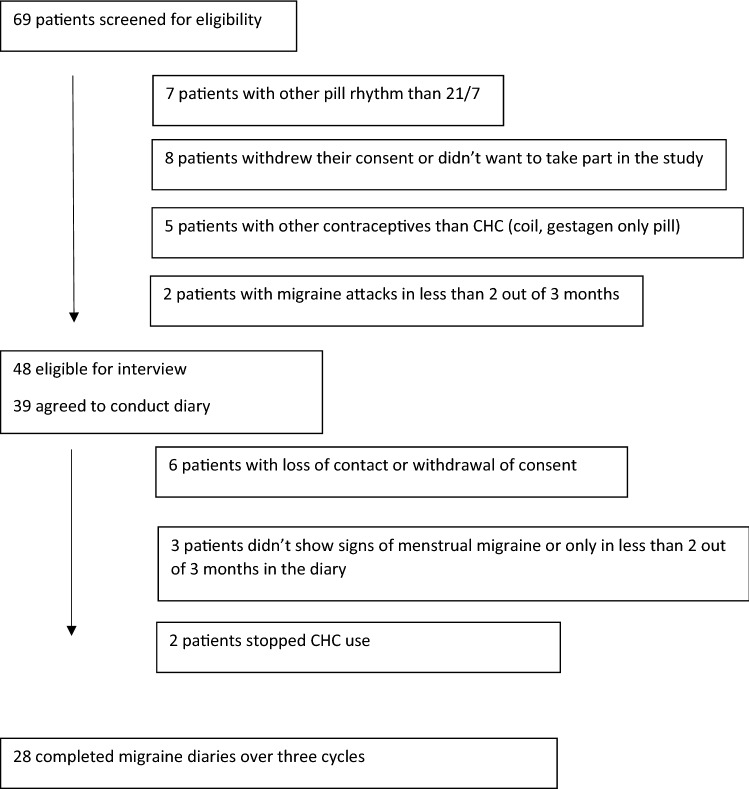
Many studies have described the features of menstrually related migraines but there is a lack of knowledge regarding the features of migraine in combined hormonal contraceptive users (CHC). Hormone-withdrawal migraines in the pill-free period could differ from those in the natural cycle. Gynaecologic comorbidities, like dysmenorrhea and endometriosis, but also depression or a family history might modify the course of migraine. A better understanding of migraine features linked to special hormonal situations could improve treatment. For this prospective cohort study, we conducted telephone interviews with women using a CHC and reporting withdrawal migraine to collect information on migraine frequency, intensity, triggers, symptoms, pain medication, gynaecologic history and comorbidities (n = 48). A subset of women agreed to also document their migraines in prospective diaries. The mean number of migraine days per cycle was 4.2 (± 2.7). Around 50% of these migraines occurred during the hormone-free interval. Migraine frequency was significantly higher in women who suffered from migraine before CHC start (5.0 ± 3.1) (n = 22) in comparison to those with migraine onset after CHC start (3.5 ± 2.1) (n = 26). Menstrually related attacks were described as more painful (57.5%), especially in women with migraine onset before CHC use (72%) (p < 0.02). Comorbidities were rare, except dysmenorrhea. The majority of migraine attacks in CHC users occur during the hormone-free interval. Similar as in the natural cycle, hormone-withdrawal migraines in CHC users are very intense and the response to acute medication is less good, especially in those women, who developed migraine before CHC use.
Keywords: Contraception; Family history; Hormone withdrawal; Menstrual migraine; Migraine.
© 2021. The Author(s).
Conflict of interest statement
GS Merki had financial relationship (lecturer, member of advisory boards and/or consultant) with Bayer, MSD, Novartis, Exeltis. These companies are not involved in the present manuscript. PS Sandor has received honoraria for advisory boards, consulting, and as a speaker, within the past 5 years, from Novartis, Eli Lilly, TEVA Pharmaceuticals, Allergan, Almirall, Amgen, MindMed, and Grünenthal. These companies are not involved in the present manuscript. RE Nappi had a financial relationship (lecturer, member of advisory boards and/or consultant) with Bayer HealthCare, Endoceutics, Exceltis, FIDIA, Gedeon Richter, MSD, Novo Nordisk, Palatin, Pfizer, Shionogi, Theramex. These companies are not involved in the present manuscript. H Pohl declares no COI. C Schankin has received honoraria from Novartis, Eli Lilly, TEVA Pharmaceuticals, Allergan, Almirall, Amgen, MindMed, and Grünenthal. These companies are not involved in the present manuscript.
Figures
Similar articles
-
Migraine start, course and features over the cycle of combined hormonal contraceptive users with menstrual migraine - temporal relation to bleeding and hormone withdrawal: a prospective diary-based study.J Headache Pain. 2020 Jun 24;21(1):81. doi: 10.1186/s10194-020-01150-1. J Headache Pain. 2020. PMID: 32580694 Free PMC article.
-
Temporal relations in hormone-withdrawal migraines and impact on prevention- a diary-based pilot study in combined hormonal contraceptive users.J Headache Pain. 2017 Aug 25;18(1):91. doi: 10.1186/s10194-017-0801-7. J Headache Pain. 2017. PMID: 28842849 Free PMC article.
-
Impact of family history for endometriosis, migraine, depression and early menopause on endometriosis symptoms, localization and stage: A case control study.Eur J Obstet Gynecol Reprod Biol. 2024 Feb;293:36-43. doi: 10.1016/j.ejogrb.2023.12.016. Epub 2023 Dec 14. Eur J Obstet Gynecol Reprod Biol. 2024. PMID: 38103542
-
Sex hormones and headache.J Pain Symptom Manage. 1993 Feb;8(2):98-114. doi: 10.1016/0885-3924(93)90107-7. J Pain Symptom Manage. 1993. PMID: 8492007 Review.
-
Sex hormones and headache.Rev Neurol (Paris). 2000;156 Suppl 4:4S30-41. Rev Neurol (Paris). 2000. PMID: 11139745 Review.
Cited by
-
Investigating migraine phenotype and dynamics in women with endometriosis: an observational pilot study.Acta Neurol Belg. 2024 Aug;124(4):1263-1271. doi: 10.1007/s13760-024-02484-2. Epub 2024 Jun 15. Acta Neurol Belg. 2024. PMID: 38878131 Free PMC article.
References
-
- Aegidius K, Zwart JA, Hagen K, et al. Oral contraceptives and increased headache prevalence: the Head-HUNT study. Neurology. 2006;66:349–353. - PubMed
-
- Allais G, Gabellari IC, De Lorenzo C, et al. Oral contraceptives in migraine. Expert Rev Neurother. 2009;9:381–393. - PubMed
-
- Loder EW, Buse DC, Golub JR. Headache as a side effect of combination estrogen-progestin oral contraceptives: a systematic review. Am J Obstet Gynecol. 2005;193:636–649. - PubMed
-
- Ferrero S, Pretta S, Bertoldi S, et al. Increased frequency of migraine among women with endometriosis. Hum Reprod. 2004;19:2927–2932. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
