

Detection and monitoring of early dental caries and erosion using three-dimensional enhanced truncated-correlation photothermal coherence tomography imaging
- PMID: 33928770
- PMCID: PMC8084349
- DOI: 10.1117/1.JBO.26.4.046004
Detection and monitoring of early dental caries and erosion using three-dimensional enhanced truncated-correlation photothermal coherence tomography imaging
Abstract
Significance: Dental caries is the most common oral disease, with significant effects on healthcare systems and quality of life. Developing diagnostic methods for early caries detection is key to reducing this burden and enabling non-invasive treatment as opposed to the drill-and-fill approach.
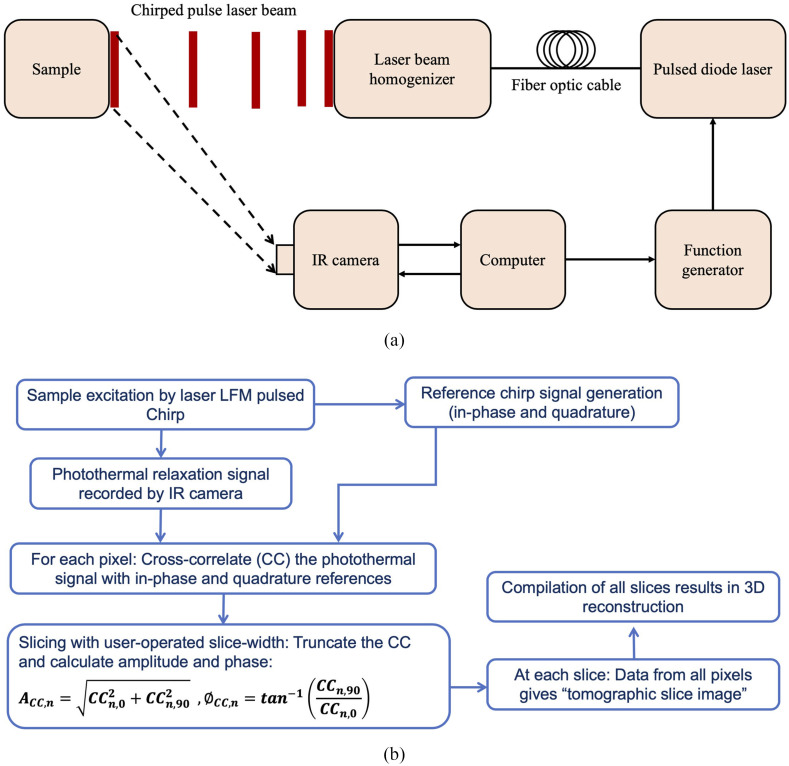
Aim: The application of a thermophotonic-based 3D imaging modality [enhanced truncated-correlation photothermal coherence tomography (eTC-PCT)] to early dental caries is investigated. To this end, the detection threshold, sensitivity, and 3D lesion reconstruction capability of eTC-PCT in imaging artificially generated caries and surface erosion are evaluated.
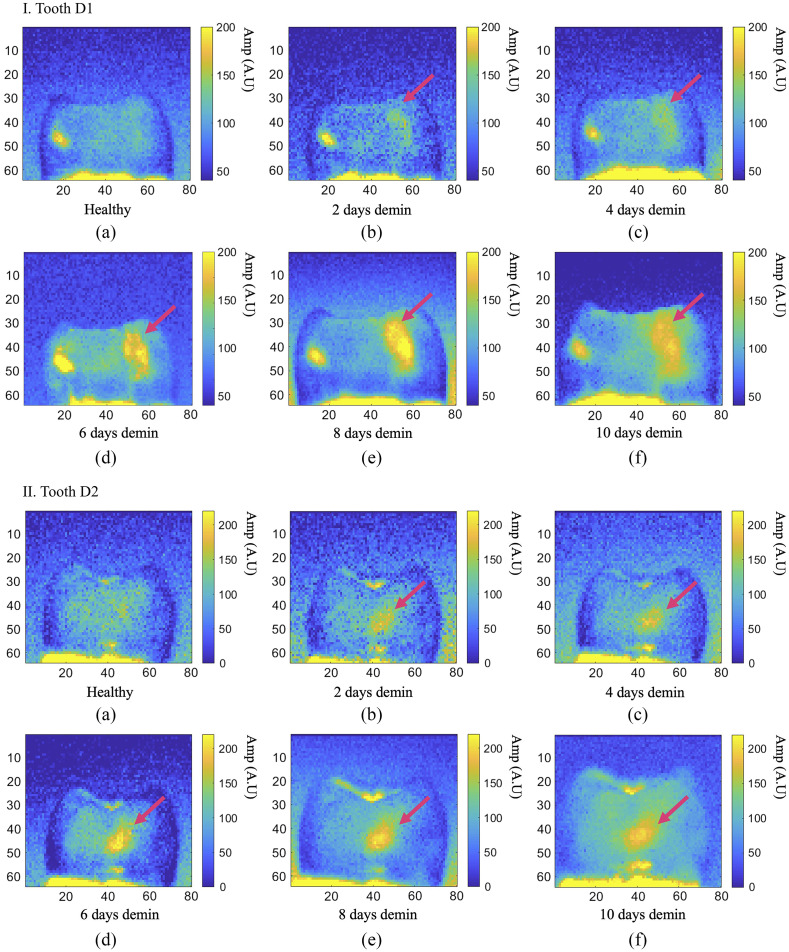
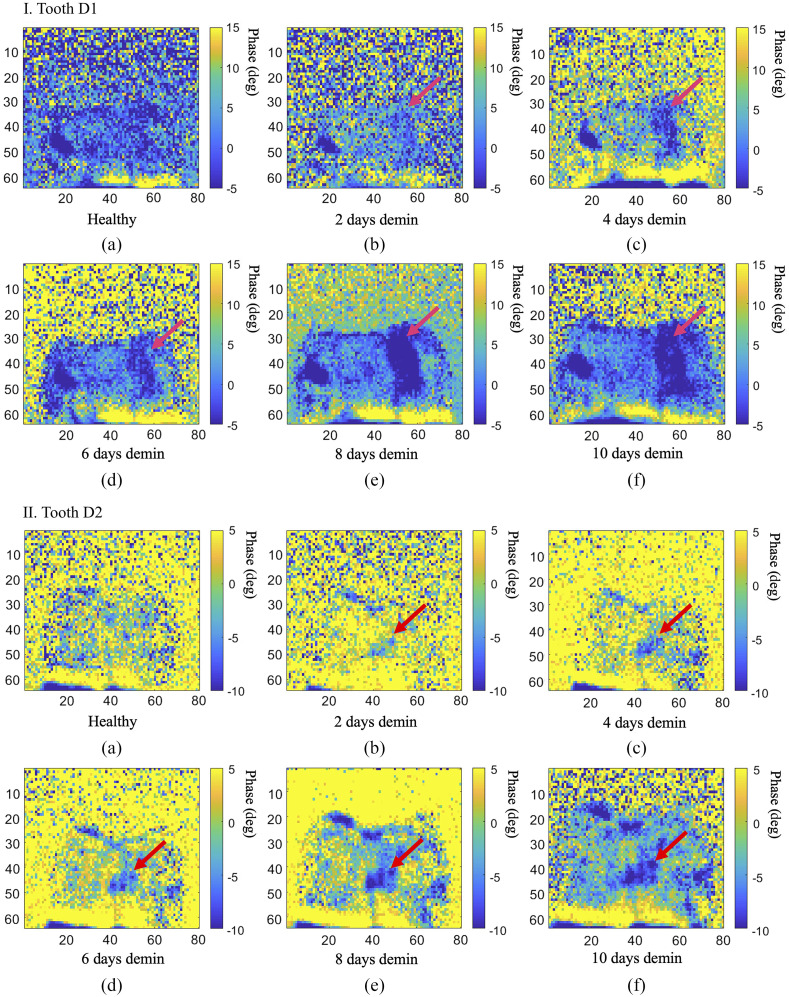
Approach: eTC-PCT employs a diode laser with pulsed excitation, a mid-IR camera, and an in-house developed image reconstruction algorithm to produce depth-resolved 2D images and 3D reconstructions. Starting with healthy teeth, dental caries and surface erosion are simulated in vitro through application of specific demineralizing/eroding acidic solutions.
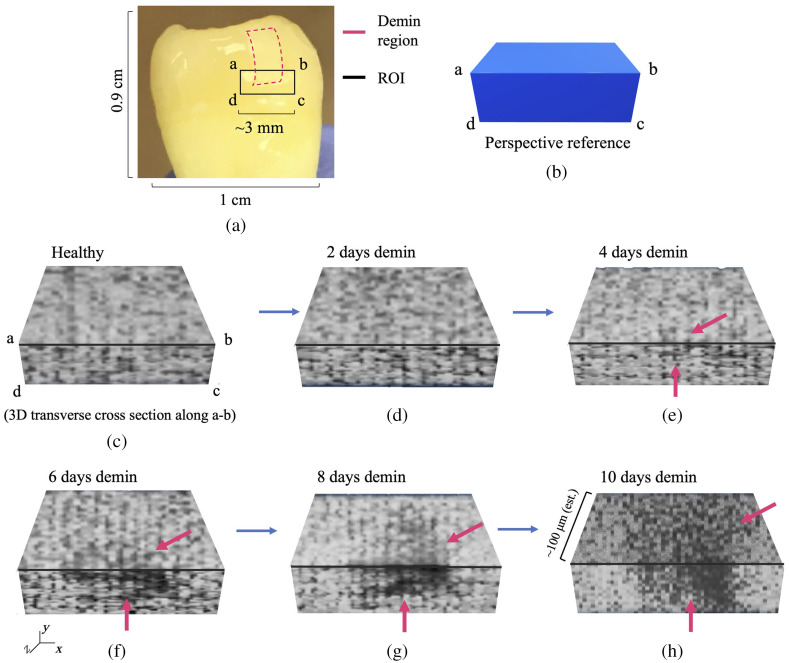
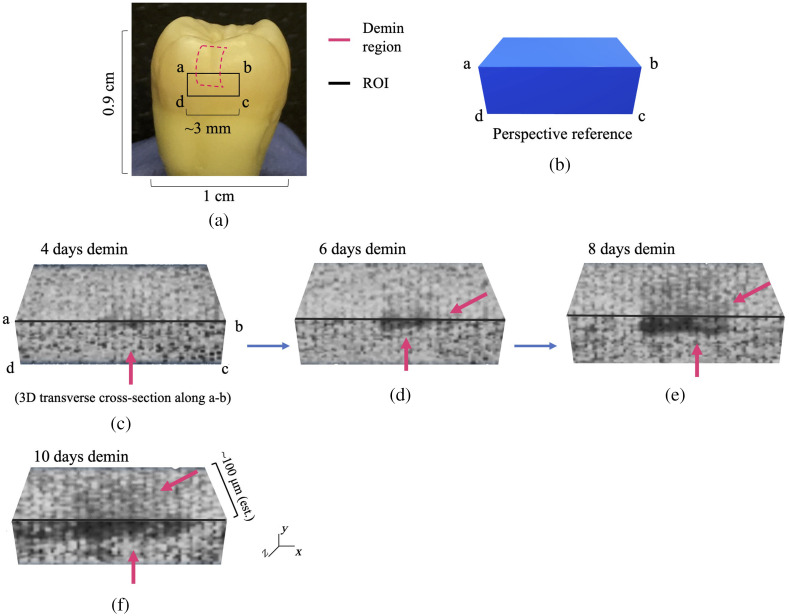
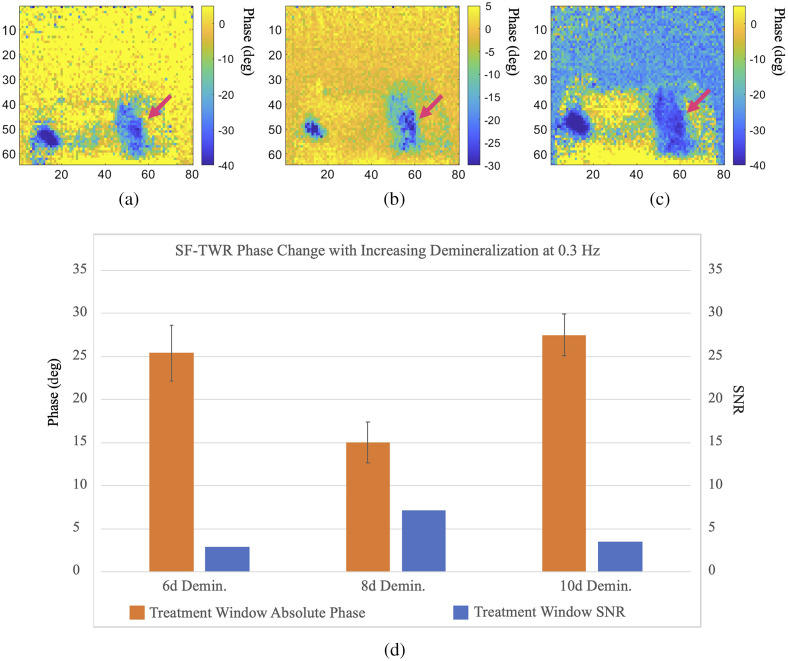
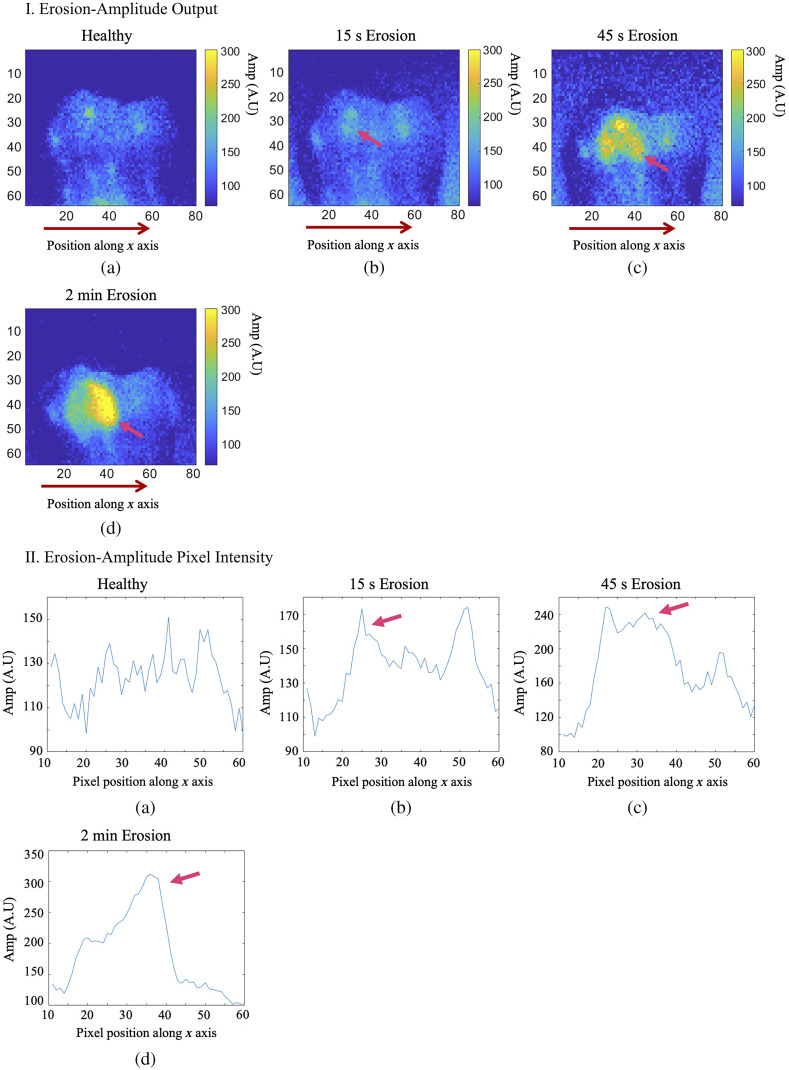
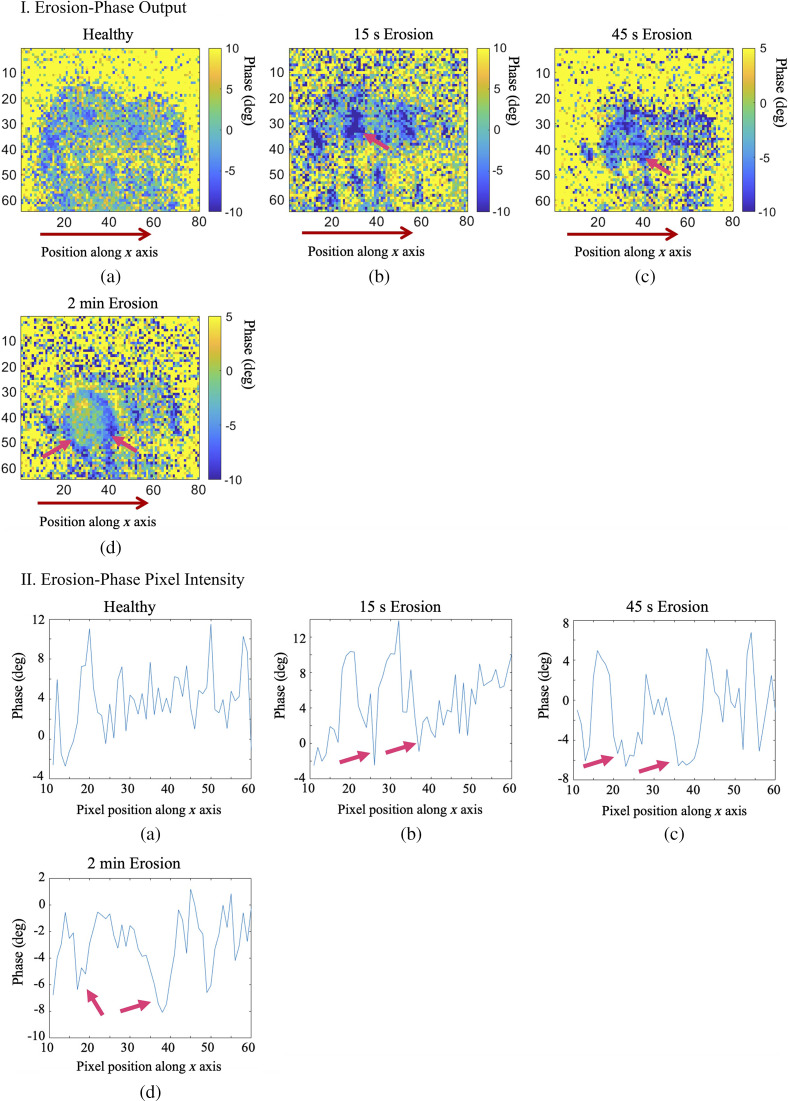
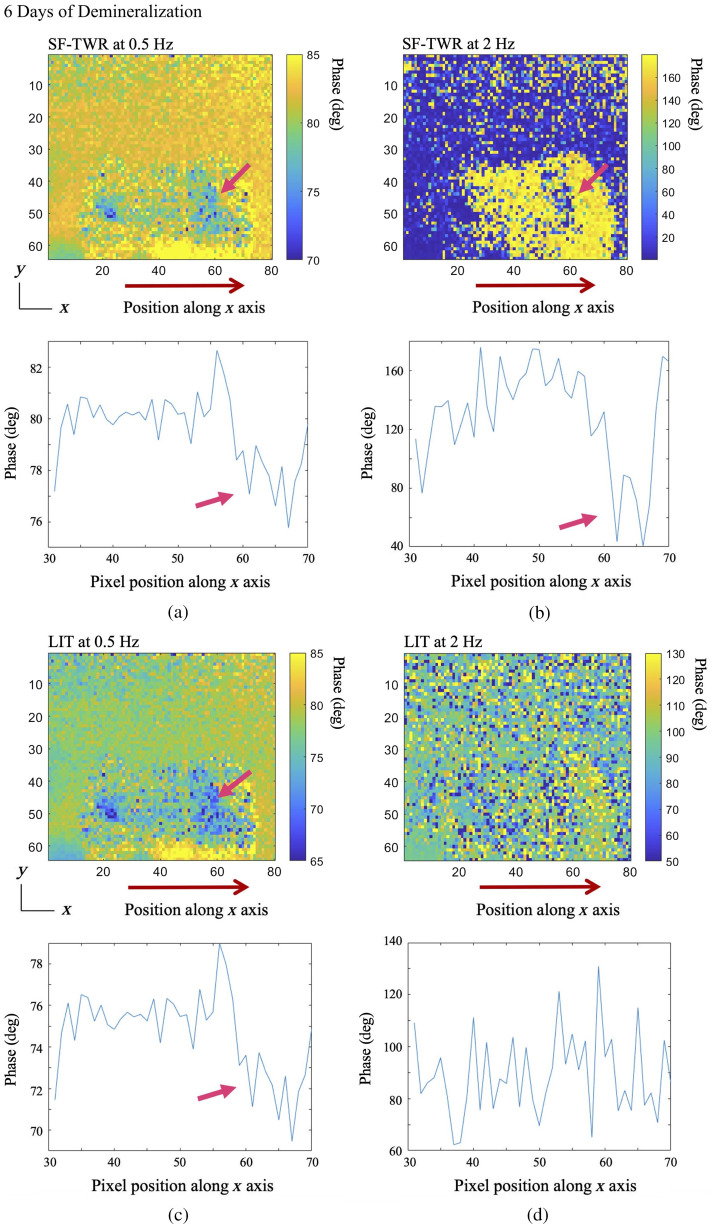
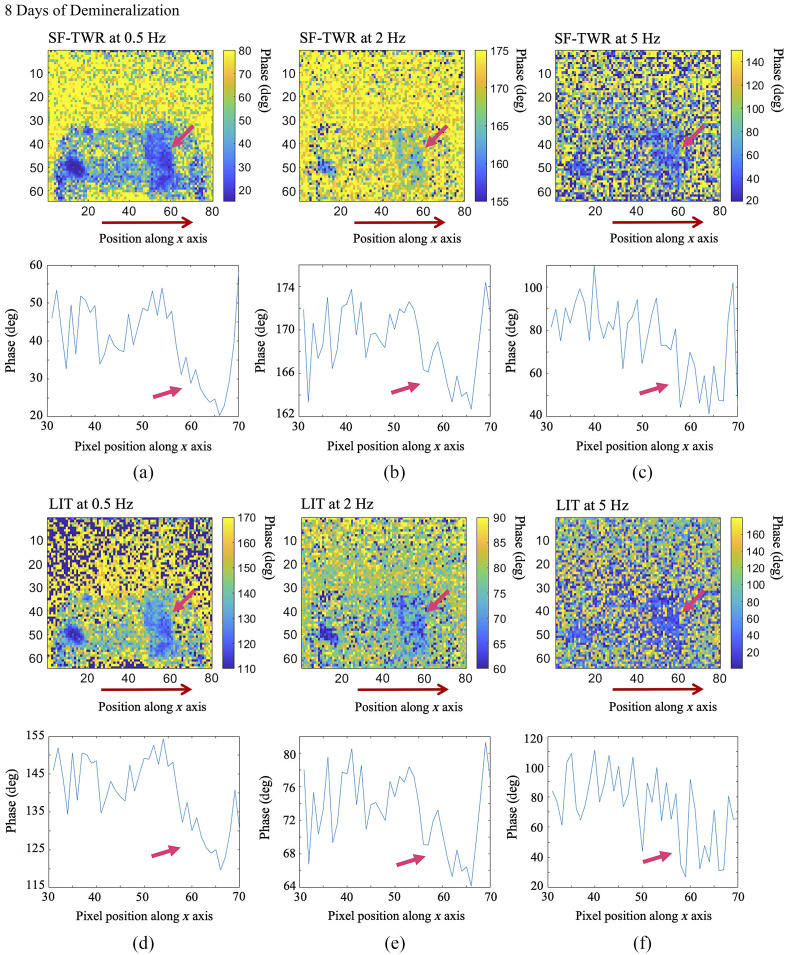
Results: eTC-PCT can detect artificial caries as early as 2 days after onset of artificial demineralization and after 45 s of surface erosion, with a laser power equivalent to 64% of maximum permissible exposure. In both cases, the lesion is not visible to the eye and undetected by x-rays. eTC-PCT is capable of monitoring lesion progression in 2-day increments and generating 3D tomographic reconstructions of the advancing lesion.
Conclusions: eTC-PCT shows great potential for further development as a dental imaging modality combining low detection threshold, high sensitivity to lesion progression, 3D reconstruction capability, and lack of ionizing radiation. These features enable early diagnosis and frequent monitoring, making eTC-PCT a promising technology for facilitating preventive dentistry.
Keywords: active thermography; dental caries detection; dental erosion detection; dental thermal imaging; enhanced truncated-correlation photothermal coherence tomography; non-invasive thermophotonic imaging.
Figures


References
-
- Technology in the National Health and Nutrition Examination Survey, “U.S. National Institute of Dental and Craniofacial Research,” 2004, http://www.nidcr.nih.gov/DataStatistics/FindDataByTopic/DentalCaries/Den....
-
- Canadian Dental Association, The State of Oral Health in Canada, “Canadian Dental Association,” pp. 1–25, 2017, https://www.cda-adc.ca/stateoforalhealth/_files/TheStateofOralHealthinCa... (accessed 21 August 2019).
-
- Ashley P., “Book review: essentials of dental caries: the disease and its management,” Primary Dental Care os13(3), 92 (2006).10.1308/135576106777795626 - DOI
-
- Jeon R. J., et al. , “Dental diagnostic clinical instrument (‘Canary’) development using photothermal radiometry and modulated luminescence,” J. Phys. Conf. Ser. 214, 012023 (2010).JPCSDZ10.1088/1742-6596/214/1/012023 - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
