

Ovary: MRI characterisation and O-RADS MRI
- PMID: 33929901
- PMCID: PMC9327753
- DOI: 10.1259/bjr.20210157
Ovary: MRI characterisation and O-RADS MRI
Abstract
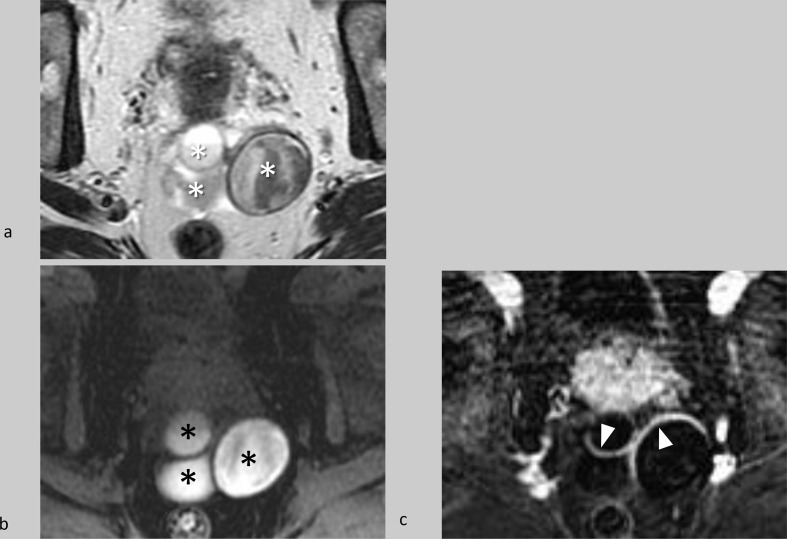
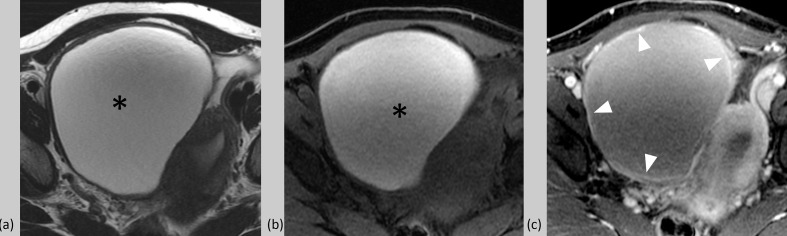
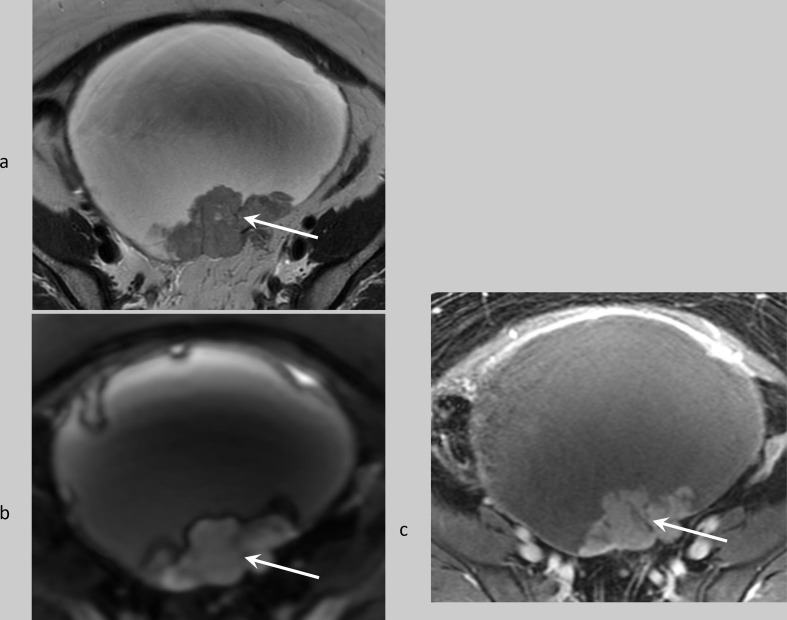
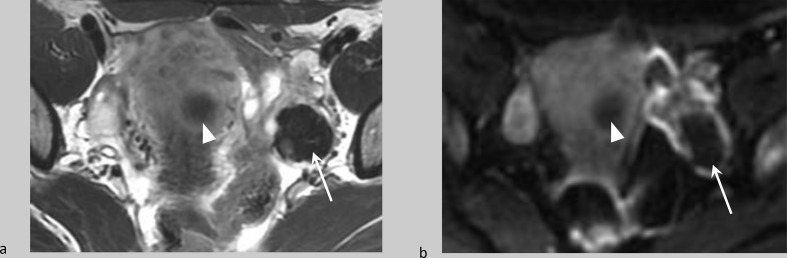
Ultrasound has a high specificity for the diagnosis of a benign lesion in cases of classic appearing simple cyst, hemorrhagic cyst, endometrioma and dermoid. However, ultrasound can sometimes be limited for definitive characterisation and risk stratification of other types of lesions, including those with echogenic content that may appear solid, with or without blood flow. Frequently, MRI can be used to further characterise these types of lesions, due to its ability to distinguish solid tissue from non-tissue solid components such as fat, blood, or debris. Incorporating the MR imaging into the evaluation of adnexal lesions can improve diagnostic certainty and guide clinical management potentially avoiding inappropriate surgery for benign lesions and expediting appropriate treatment for malignant lesions, particularly in the females with sonographically indeterminate adnexal lesions.
Figures
References
-
- Buys SS, Partridge E, Greene MH, Prorok PC, Reding D, Riley TL, et al. Ovarian cancer screening in the prostate, lung, colorectal and ovarian (PLCO) cancer screening trial: findings from the initial screen of a randomized trial. Am J Obstet Gynecol 2005; 193: 1630–9. doi: 10.1016/j.ajog.2005.05.005 - DOI - PubMed
-
- Greenlee RT, Kessel B, Williams CR, Riley TL, Ragard LR, Hartge P, et al. Prevalence, incidence, and natural history of simple ovarian cysts among women >55 years old in a large cancer screening trial. Am J Obstet Gynecol 2010; 202: 373.e1–373.e9. doi: 10.1016/j.ajog.2009.11.029 - DOI - PMC - PubMed
-
- Sharma A, Apostolidou S, Burnell M, Campbell S, Habib M, Gentry-Maharaj A, et al. Risk of epithelial ovarian cancer in asymptomatic women with ultrasound-detected ovarian masses: a prospective cohort study within the UK Collaborative trial of ovarian cancer screening (UKCTOCS. Ultrasound Obstet Gynecol 2012; 40: 338–44. doi: 10.1002/uog.12270 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
