

COVID-19-associated coagulopathy and antithrombotic agents-lessons after 1 year
- PMID: 33930350
- PMCID: PMC8078884
- DOI: 10.1016/S2352-3026(21)00105-8
COVID-19-associated coagulopathy and antithrombotic agents-lessons after 1 year
Abstract
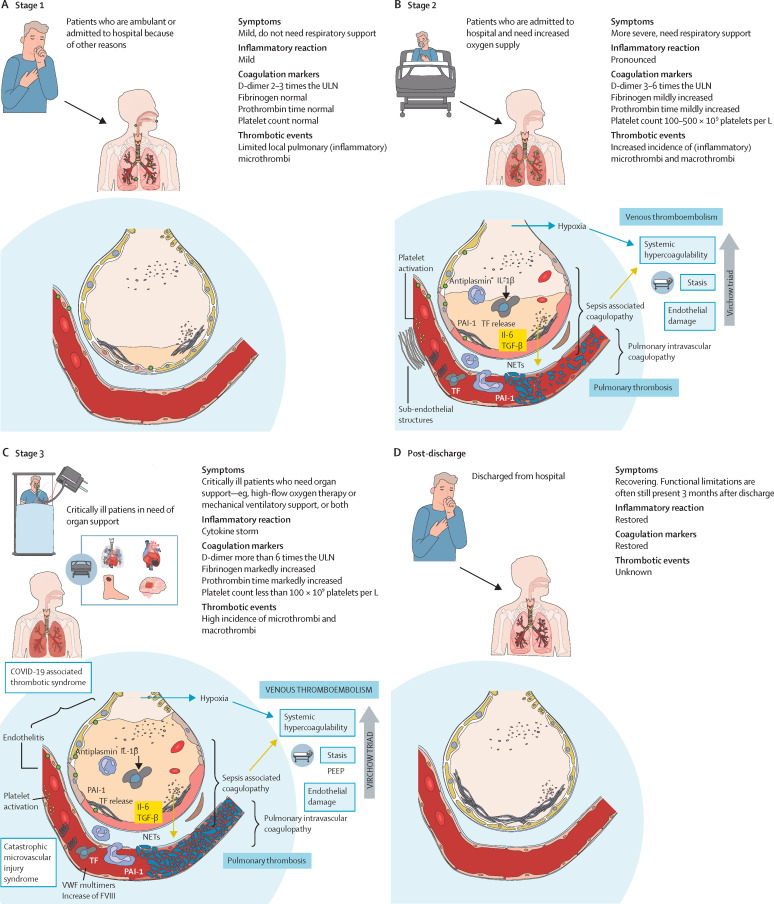
COVID-19 is associated with a high incidence of thrombotic complications, which can be explained by the complex and unique interplay between coronaviruses and endothelial cells, the local and systemic inflammatory response, and the coagulation system. Empirically, an intensified dose of thrombosis prophylaxis is being used in patients admitted to hospital with COVID-19 and several guidelines on this topic have been published, although the insufficiency of high quality and direct evidence has led to weak recommendations. In this Viewpoint we summarise the pathophysiology of COVID-19 coagulopathy in the context of patients who are ambulant, admitted to hospital, and critically ill or non-critically ill, and those post-discharge from hospital. We also review data from randomised controlled trials in the past year of antithrombotic therapy in patients who are critically ill. These data provide the first high-quality evidence on optimal use of antithrombotic therapy in patients with COVID-19. Pharmacological thromboprophylaxis is not routinely recommended for patients who are ambulant and post-discharge. A first ever trial in non-critically ill patients who were admitted to hospital has shown that a therapeutic dose of low-molecular-weight heparin might improve clinical outcomes in this population. In critically ill patients, this same treatment does not improve outcomes and prophylactic dose anticoagulant thromboprophylaxis is recommended. In the upcoming months we expect numerous data from the ongoing antithrombotic COVID-19 studies to guide clinicians at different stages of the disease.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests JL and TFvH declare no competing interests. PFW reports personal fees from Sanofi, Bayer, Boehringer Ingelheim, Pfizer, and Sandoz. REGS reports grants from CSL Behring, Pfizer, Sanquin, and Sobi; grants and personal fees from Bayer and Novonordisk; and is a member of the scientific advisory board of Freeline, Boehringer Ingelheim, Roche, and Sobi. SM reports grants and personal fees from Daiichi Sankyo, Bayer, Pfizer, and Boehringer Ingelheim; and personal fees from Portola, Abbvie, and Bristol-Myers Squibb-Pfizer. SM is a steering committee member of the RAPID COVID COAG trial. SM and REGS are members of the anticoagulation domain of the REMAP-CAP trial.
Figures
Comment in
-
Sustained prothrombotic changes in convalescent patients with COVID-19.Lancet Haematol. 2021 Jul;8(7):e475. doi: 10.1016/S2352-3026(21)00146-0. Lancet Haematol. 2021. PMID: 34171275 Free PMC article. No abstract available.
References
-
- Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): a review. JAMA. 2020;324:782–793. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
