

Association of changes of pulse wave velocity and augmentation index after isometric handgrip exercise with coronary lesion extent and revascularization
- PMID: 33931135
- PMCID: PMC8088004
- DOI: 10.1186/s40885-021-00163-5
Association of changes of pulse wave velocity and augmentation index after isometric handgrip exercise with coronary lesion extent and revascularization
Abstract
Background: Arterial stiffness is associated with myocardial ischemia and incident coronary artery disease (CAD), and indexes of arterial stiffness are usually increased in patients with CAD. However, these indexes are often increased in elderly without CAD. Arterial stiffness in patients with CAD may become more evident after isometric handgrip exercise which increases systolic pressure and ventricular afterload. We investigated the association of the change of stiffness indexes after isometric handgrip exercise with the lesion extent of CAD and the necessity for coronary revascularization.
Methods: Patients who were scheduled a routine coronary angiography via a femoral artery were enrolled. Arterial waveforms were traced at aortic root and external iliac artery using coronary catheters at baseline and 3 min after handgrip exercise. Augmentation index (AIx) was measured on the recorded aortic pressure waveform, and pulse wave velocity (PWV) was calculated using the ECG-gated time difference of the upstroke of arterial waveforms and distance between aortic root and external iliac artery.
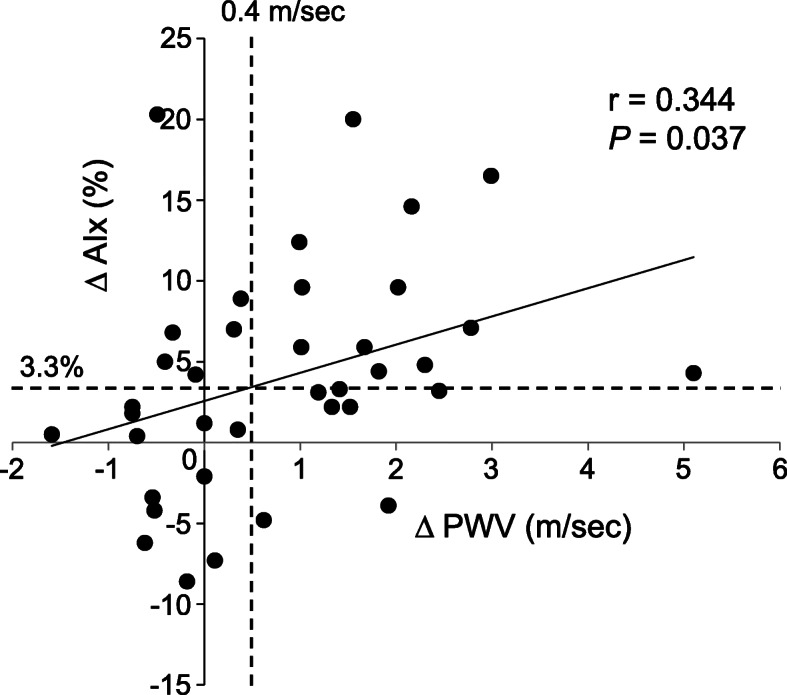
Results: Total 37 patients were evaluated. Both PWV and AIx increased after handgrip exercise. ΔPWV was significantly correlated with ΔAIx (r = 0.344, P = 0.037). Patients were divided into higher and lower ΔPWV or ΔAIx groups based on the median values of 0.4 m/sec and 3.3%, respectively. Patients with higher PWV had more 2- or 3-vessel CAD (69% vs. 27%, P = 0.034), and underwent percutaneous coronary intervention (PCI) more frequently (84% vs. 50%, P = 0.038), but higher ΔAIx was not associated with either the lesion extent or PCI. Area under curve (AUC) of ΔPWV in association with PCI by C-statistics was 0.70 (95% confidence interval [CI] 0.51-0.88; P = 0.056). In multiple logistic regression analysis, ΔPWV was significantly associated with PCI (odds ratio 7.78; 95% CI 1.26-48.02; P = 0.027).
Conclusions: Higher ΔPWV after isometric handgrip exercise was associated with the lesion extent of CAD and the necessity for coronary revascularization, but higher ΔAIx was not.
Keywords: Arterial stiffness; Isometric exercise; Percutaneous coronary intervention; Pulse wave analysis; Pulse wave velocity.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Nichols WW, O’Rourke MF, Vlachopoulos C. McDonald’s blood flow in arteries. 6. Boca Raton: CRC Press; 2011. Wave reflection; pp. 195–223.
-
- Ikonomidis I, Makavos G, Lekakis J. Arterial stiffness and coronary artery disease. Curr Opin Cardiol. 2015;30:422–431. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous