

Expanded antigen-experienced CD160+CD8+effector T cells exhibit impaired effector functions in chronic lymphocytic leukemia
- PMID: 33931471
- PMCID: PMC8098955
- DOI: 10.1136/jitc-2020-002189
Expanded antigen-experienced CD160+CD8+effector T cells exhibit impaired effector functions in chronic lymphocytic leukemia
Abstract
Background: T cell exhaustion compromises antitumor immunity, and a sustained elevation of co-inhibitory receptors is a hallmark of T cell exhaustion in solid tumors. Similarly, upregulation of co-inhibitory receptors has been reported in T cells in hematological cancers such as chronic lymphocytic leukemia (CLL). However, the role of CD160, a glycosylphosphatidylinositol-anchored protein, as one of these co-inhibitory receptors has been contradictory in T cell function. Therefore, we decided to elucidate how CD160 expression and/or co-expression with other co-inhibitory receptors influence T cell effector functions in patients with CLL.
Methods: We studied 56 patients with CLL and 25 age-matched and sex-matched healthy controls in this study. The expression of different co-inhibitory receptors was analyzed in T cells obtained from the peripheral blood or the bone marrow. Also, we quantified the properties of extracellular vesicles (EVs) in the plasma of patients with CLL versus healthy controls. Finally, we measured 29 different cytokines, chemokines or other biomarkers in the plasma specimens of patients with CLL and healthy controls.
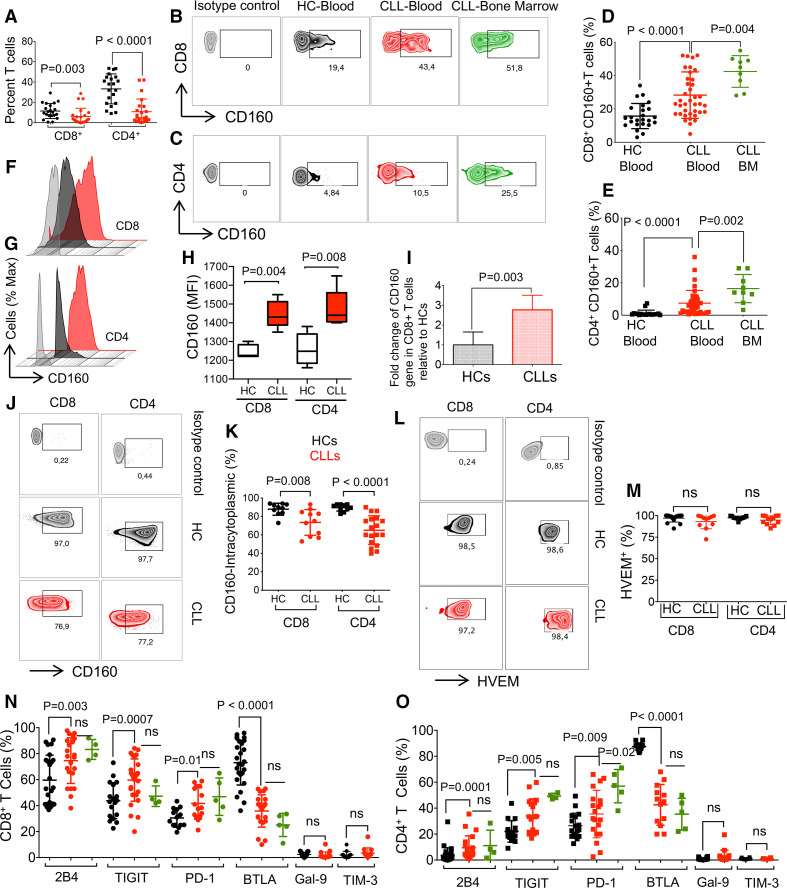
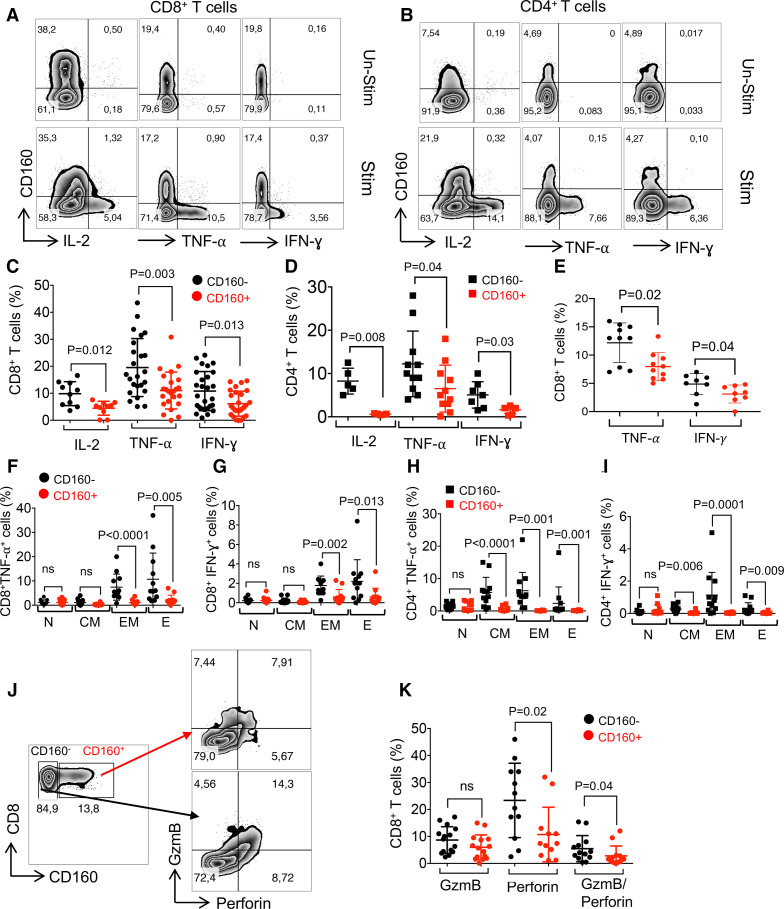
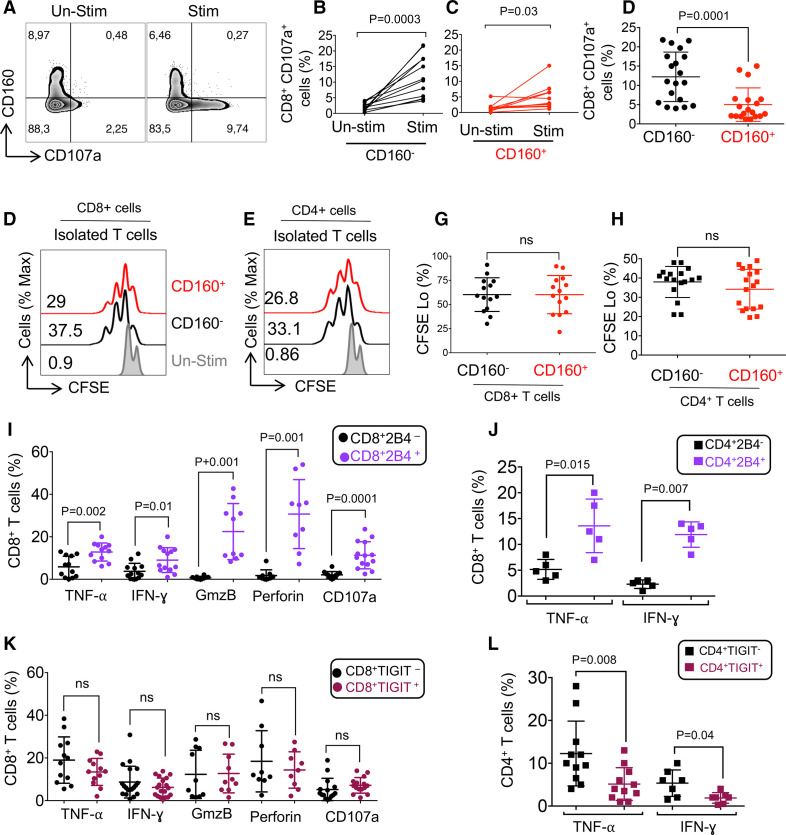
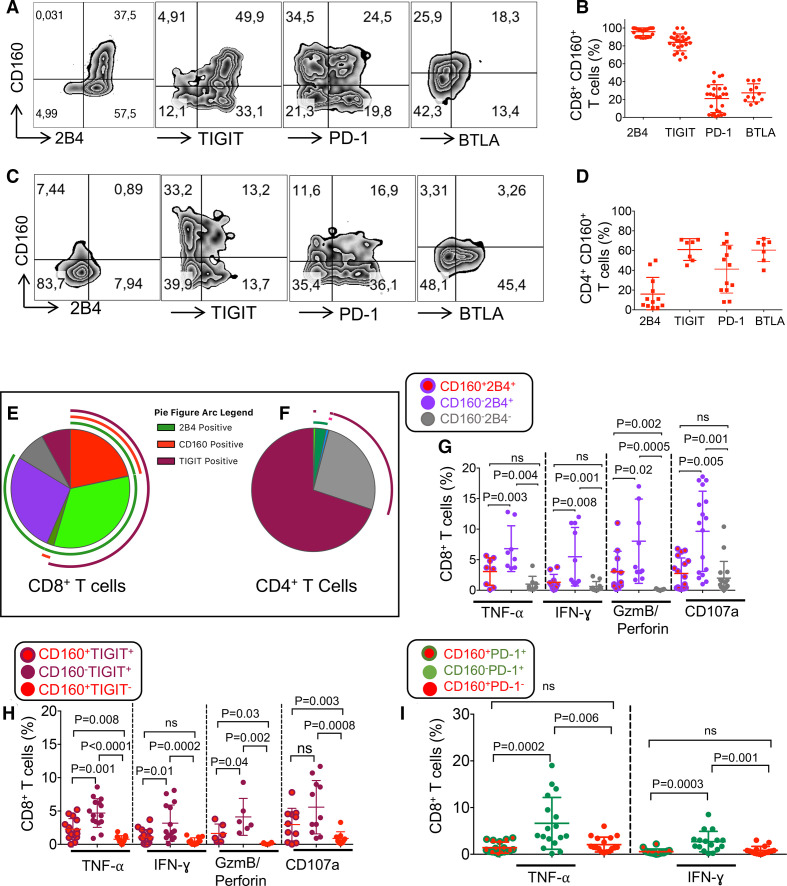
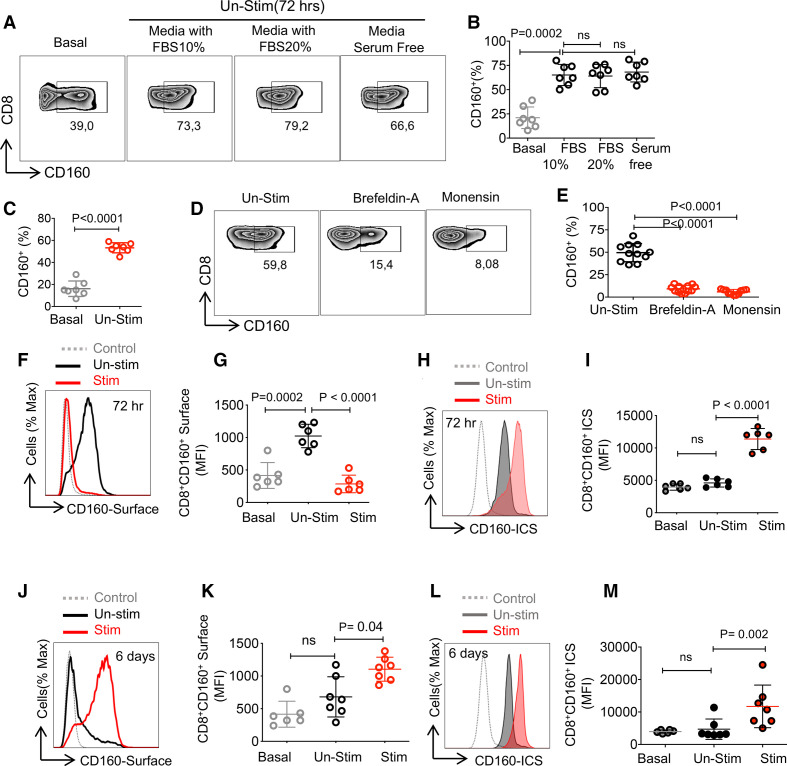
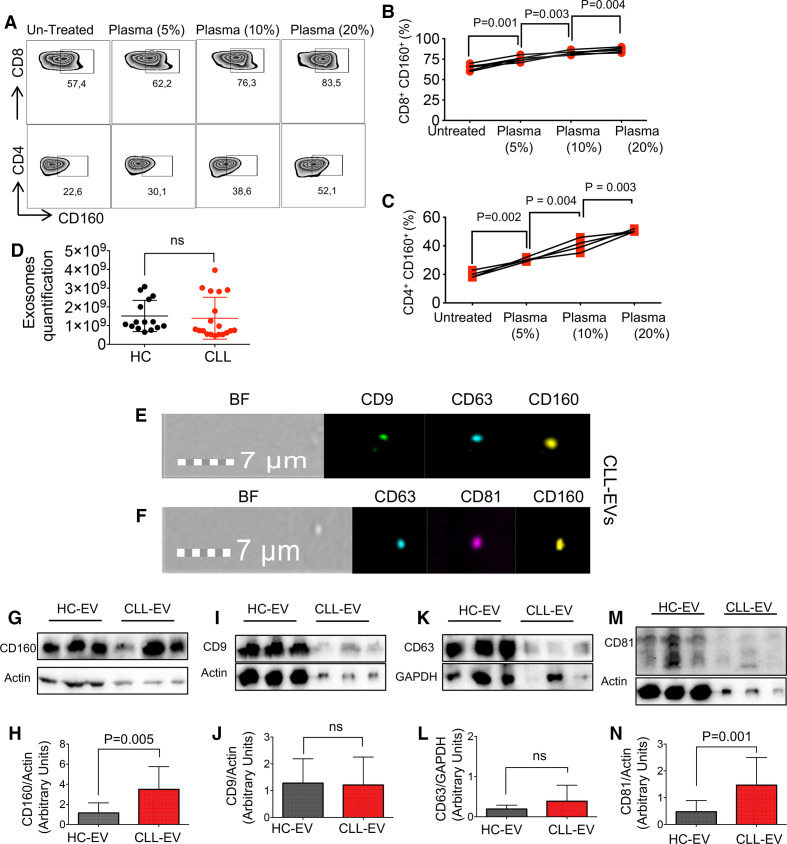
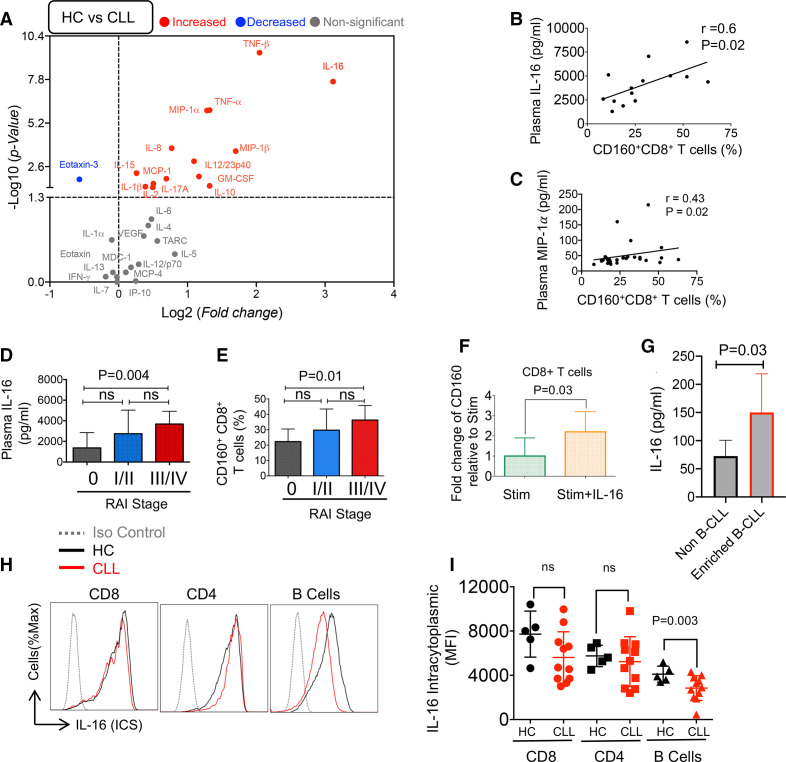
Results: We found that CD160 was the most upregulated co-inhibitory receptor in patients with CLL. Its expression was associated with an exhausted T cell phenotype. CD160+CD8+ T cells were highly antigen-experienced/effector T cells, while CD160+CD4+ T cells were more heterogeneous. In particular, we identified EVs as a source of CD160 in the plasma of patients with CLL that can be taken up by T cells. Moreover, we observed a dominantly proinflammatory cytokine profile in the plasma of patients with CLL. In particular, interleukin-16 (IL-16) was highly elevated and correlated with the advanced clinical stage (Rai). Furthermore, we observed that the incubation of T cells with IL-16 results in the upregulation of CD160.
Conclusions: Our study provides a novel insight into the influence of CD160 expression/co-expression with other co-inhibitory receptors in T cell effector functions in patients with CLL. Besides, IL-16-mediated upregulation of CD160 expression in T cells highlights the importance of IL-16/CD160 as potential immunotherapy targets in patients with CLL. Therefore, our findings propose a significant role for CD160 in T cell exhaustion in patients with CLL.
Keywords: B-lymphocytes; T-lymphocytes; cellular; costimulatory and inhibitory T-cell receptors; cytokines; immunity.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
CD160 receptor in CLL: Current state and future avenues.Front Immunol. 2022 Nov 7;13:1028013. doi: 10.3389/fimmu.2022.1028013. eCollection 2022. Front Immunol. 2022. PMID: 36420268 Free PMC article. Review.
-
T cells from CLL patients exhibit features of T-cell exhaustion but retain capacity for cytokine production.Blood. 2013 Feb 28;121(9):1612-21. doi: 10.1182/blood-2012-09-457531. Epub 2012 Dec 17. Blood. 2013. PMID: 23247726 Free PMC article.
-
CD160 signaling mediates PI3K-dependent survival and growth signals in chronic lymphocytic leukemia.Blood. 2010 Apr 15;115(15):3079-88. doi: 10.1182/blood-2009-08-239483. Epub 2010 Feb 17. Blood. 2010. PMID: 20164468 Free PMC article.
-
Polyfunctional CD8+CD226+RUNX2hi effector T cells are diminished in advanced stages of chronic lymphocytic leukemia.Mol Oncol. 2025 May;19(5):1347-1370. doi: 10.1002/1878-0261.13793. Epub 2025 Jan 7. Mol Oncol. 2025. PMID: 39777847 Free PMC article.
-
T-cells in chronic lymphocytic leukemia: Guardians or drivers of disease?Leukemia. 2020 Aug;34(8):2012-2024. doi: 10.1038/s41375-020-0873-2. Epub 2020 May 26. Leukemia. 2020. PMID: 32457353 Free PMC article. Review.
Cited by
-
CD160 receptor in CLL: Current state and future avenues.Front Immunol. 2022 Nov 7;13:1028013. doi: 10.3389/fimmu.2022.1028013. eCollection 2022. Front Immunol. 2022. PMID: 36420268 Free PMC article. Review.
-
CD160 dictates anti-PD-1 immunotherapy resistance by regulating CD8+ T cell exhaustion in colorectal cancer.Nat Cell Biol. 2025 Sep 9. doi: 10.1038/s41556-025-01753-3. Online ahead of print. Nat Cell Biol. 2025. PMID: 40925954
-
Depletion of polyfunctional CD26highCD8+ T cells repertoire in chronic lymphocytic leukemia.Exp Hematol Oncol. 2023 Jan 27;12(1):13. doi: 10.1186/s40164-023-00375-5. Exp Hematol Oncol. 2023. PMID: 36707896 Free PMC article.
-
Differential Signature of the Microbiome and Neutrophils in the Oral Cavity of HIV-Infected Individuals.Front Immunol. 2021 Nov 9;12:780910. doi: 10.3389/fimmu.2021.780910. eCollection 2021. Front Immunol. 2021. PMID: 34858437 Free PMC article.
-
Hematopoietic responses to SARS-CoV-2 infection.Cell Mol Life Sci. 2022 Mar 13;79(3):187. doi: 10.1007/s00018-022-04220-6. Cell Mol Life Sci. 2022. PMID: 35284964 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous