

Associations between body-mass index and COVID-19 severity in 6·9 million people in England: a prospective, community-based, cohort study
- PMID: 33932335
- PMCID: PMC8081400
- DOI: 10.1016/S2213-8587(21)00089-9
Associations between body-mass index and COVID-19 severity in 6·9 million people in England: a prospective, community-based, cohort study
Abstract
Background: Obesity is a major risk factor for adverse outcomes after infection with SARS-CoV-2. We aimed to examine this association, including interactions with demographic and behavioural characteristics, type 2 diabetes, and other health conditions.
Methods: In this prospective, community-based, cohort study, we used de-identified patient-level data from the QResearch database of general practices in England, UK. We extracted data for patients aged 20 years and older who were registered at a practice eligible for inclusion in the QResearch database between Jan 24, 2020 (date of the first recorded infection in the UK) and April 30, 2020, and with available data on BMI. Data extracted included demographic, clinical, clinical values linked with Public Health England's database of positive SARS-CoV-2 test results, and death certificates from the Office of National Statistics. Outcomes, as a proxy measure of severe COVID-19, were admission to hospital, admission to an intensive care unit (ICU), and death due to COVID-19. We used Cox proportional hazard models to estimate the risk of severe COVID-19, sequentially adjusting for demographic characteristics, behavioural factors, and comorbidities.
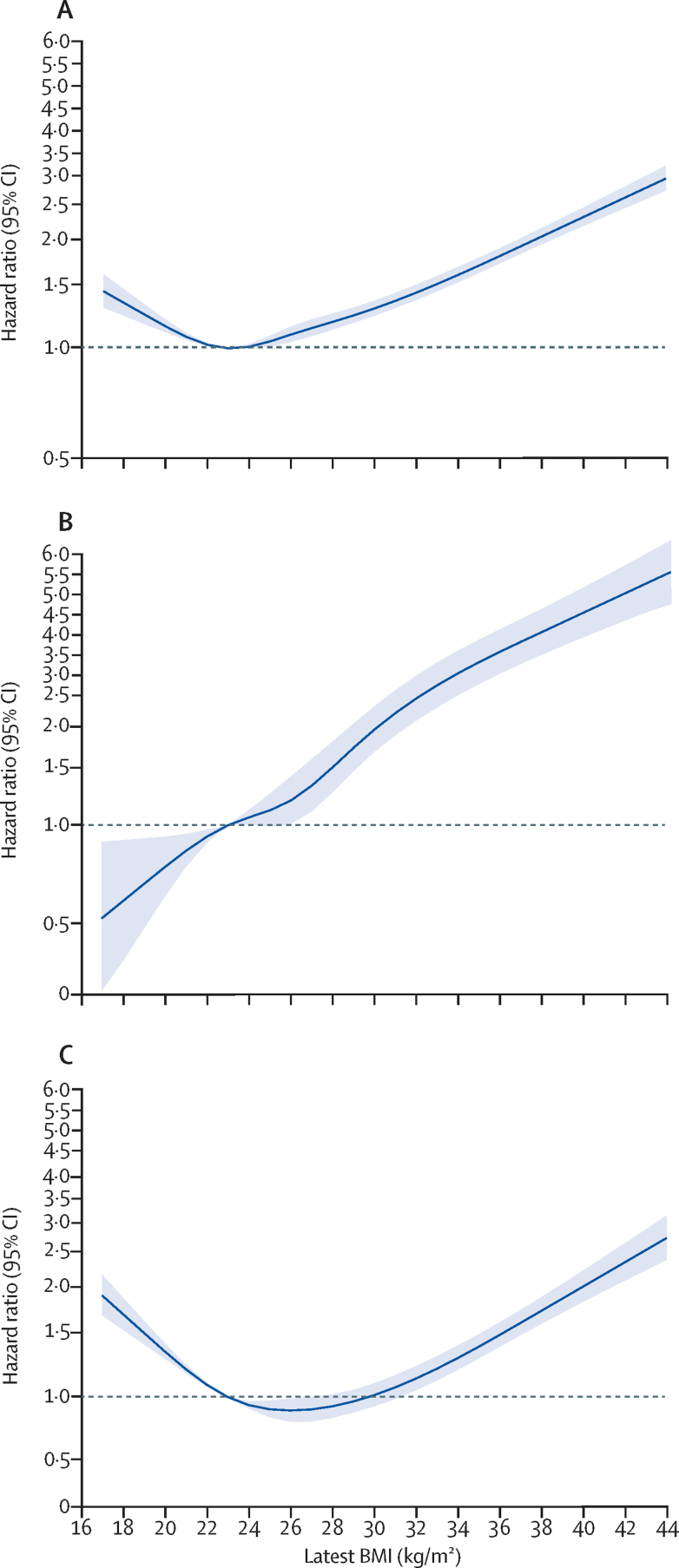
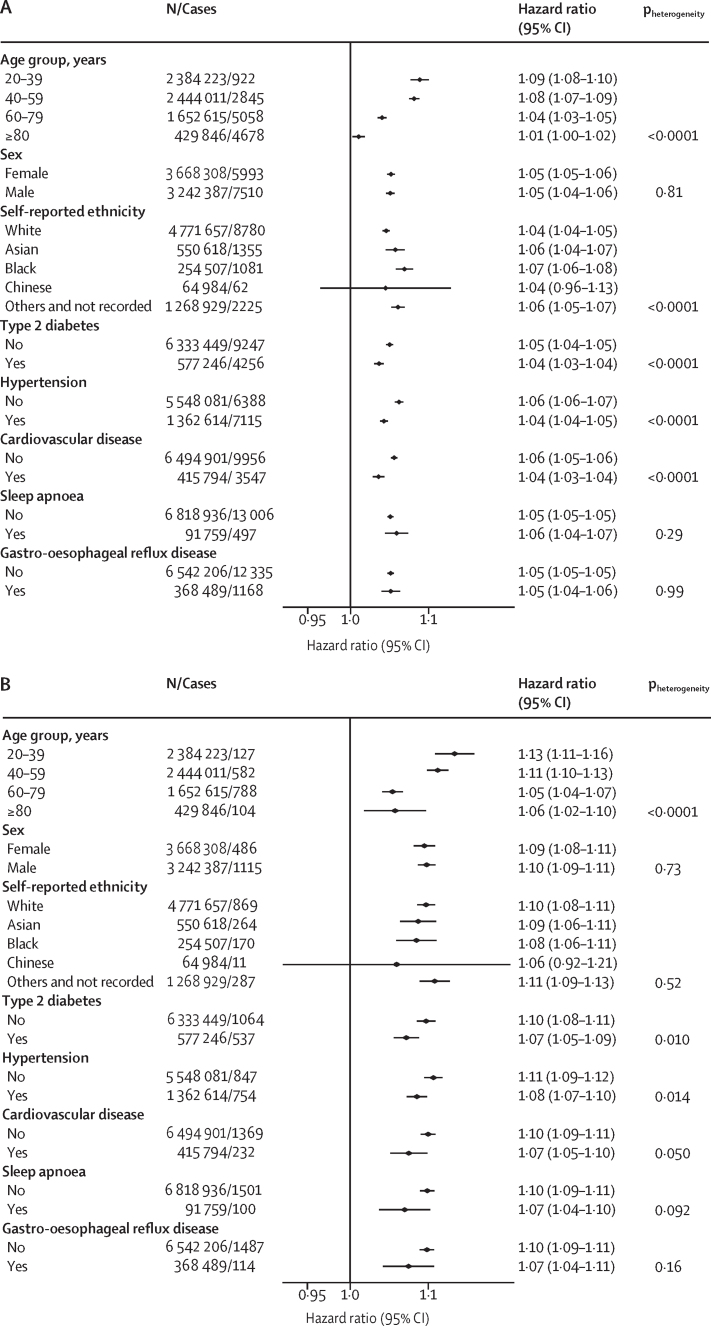
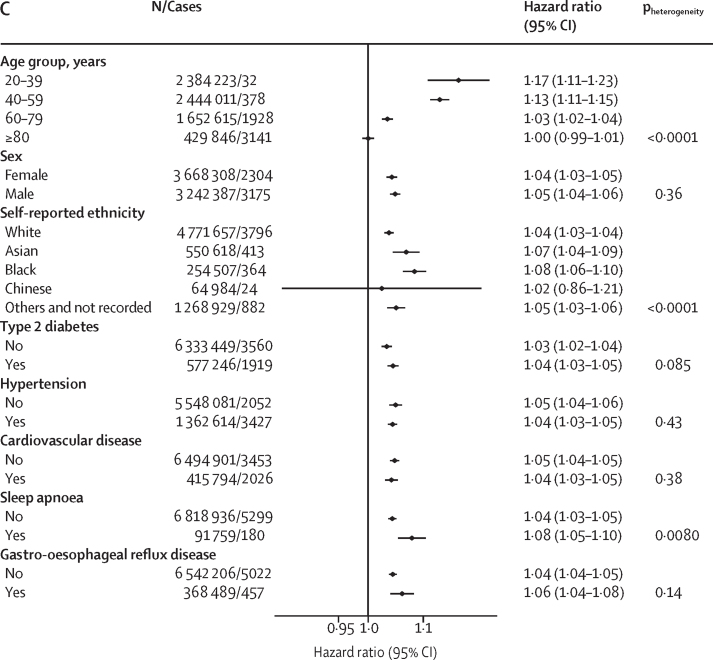
Findings: Among 6 910 695 eligible individuals (mean BMI 26·78 kg/m2 [SD 5·59]), 13 503 (0·20%) were admitted to hospital, 1601 (0·02%) to an ICU, and 5479 (0·08%) died after a positive test for SARS-CoV-2. We found J-shaped associations between BMI and admission to hospital due to COVID-19 (adjusted hazard ratio [HR] per kg/m2 from the nadir at BMI of 23 kg/m2 of 1·05 [95% CI 1·05-1·05]) and death (1·04 [1·04-1·05]), and a linear association across the whole BMI range with ICU admission (1·10 [1·09-1·10]). We found a significant interaction between BMI and age and ethnicity, with higher HR per kg/m2 above BMI 23 kg/m2 for younger people (adjusted HR per kg/m2 above BMI 23 kg/m2 for hospital admission 1·09 [95% CI 1·08-1·10] in 20-39 years age group vs 80-100 years group 1·01 [1·00-1·02]) and Black people than White people (1·07 [1·06-1·08] vs 1·04 [1·04-1·05]). The risk of admission to hospital and ICU due to COVID-19 associated with unit increase in BMI was slightly lower in people with type 2 diabetes, hypertension, and cardiovascular disease than in those without these morbidities.
Interpretation: At a BMI of more than 23 kg/m2, we found a linear increase in risk of severe COVID-19 leading to admission to hospital and death, and a linear increase in admission to an ICU across the whole BMI range, which is not attributable to excess risks of related diseases. The relative risk due to increasing BMI is particularly notable people younger than 40 years and of Black ethnicity.
Funding: NIHR Oxford Biomedical Research Centre.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests NMA, PA, and SAJ were investigators on a trial of total diet replacement for weight loss funded by a grant from Cambridge Weight Plan UK to the University of Oxford (Oxford, UK) and received no personal payments from this. PA spoke at a symposium at the Royal College of General Practitioners annual conference on interventions for weight loss that was funded by Novo Nordisk and received no personal payments. JH-C reports grants from National Institute for Health Research (NIHR) Oxford Biomedical Research Centre (BRC), John Fell Oxford University Press Research Fund, Cancer Research UK (C5255/A18085) through the Cancer Research UK Oxford Centre, and Oxford Wellcome Institutional Strategic Support Fund (204826/Z/16/Z) during the conduct of the study. JH-C received personal fees and other support from ClinRisk (until 2019) outside of the submitted work, and is an unpaid director of QResearch, a not-for-profit organisation that is a partnership between the University of Oxford and Egton Medical Information Systems (EMIS) Health who supply the QResearch database used for this work. All other authors declare no competing interests.
Figures
Comment in
-
New insights into the association between body-mass index and severe COVID-19.Lancet Diabetes Endocrinol. 2021 Jun;9(6):322-323. doi: 10.1016/S2213-8587(21)00109-1. Epub 2021 Apr 28. Lancet Diabetes Endocrinol. 2021. PMID: 33932336 Free PMC article. No abstract available.
-
People carrying excess weight have an increased risk of severe covid-19.BMJ. 2022 Feb 2;376:o141. doi: 10.1136/bmj.o141. BMJ. 2022. PMID: 35110298
References
-
- Peng YD, Meng K, Guan HQ. Clinical characteristics and outcomes of 112 cardiovascular disease patients infected by 2019-nCoV. Zhonghua Xin Xue Guan Bing Za Zhi. 2020;48:e004. (in Chinese). - PubMed
-
- Wu J, Li W, Shi X. Early antiviral treatment contributes to alleviate the severity and improve the prognosis of patients with novel coronavirus disease (COVID-19) J Intern Med. 2020;288:128–138. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
