

Asymptomatic malaria and anaemia among pregnant women during high and low malaria transmission seasons in Burkina Faso: household-based cross-sectional surveys in Burkina Faso, 2013 and 2017
- PMID: 33933072
- PMCID: PMC8088076
- DOI: 10.1186/s12936-021-03703-4
Asymptomatic malaria and anaemia among pregnant women during high and low malaria transmission seasons in Burkina Faso: household-based cross-sectional surveys in Burkina Faso, 2013 and 2017
Abstract
Background: Malaria in endemic countries is often asymptomatic during pregnancy, but it has substantial consequences for both the mother and her unborn baby. During pregnancy, anaemia is an important consequence of malaria infection. In Burkina Faso, the intensity of malaria varies according to the season, albeit the prevalence of malaria and anaemia as well as their risk factors, during high and low malaria transmission seasons is underexplored at the household level.
Methods: Data of 1751 pregnant women from October 2013 to March 2014 and 1931 pregnant women from April 2017 to June 2017 were drawn from two cross-sectional household surveys conducted in 24 health districts of Burkina Faso. Pregnant women were tested for malaria in their household after consenting. Asymptomatic carriage was defined as a positive result from malaria rapid diagnostic tests in the absence of clinical symptoms of malaria. Anaemia was defined as haemoglobin level less than 11 g/dL in the first and third trimester and less than 10.5 g/dL in the second trimester of pregnancy.
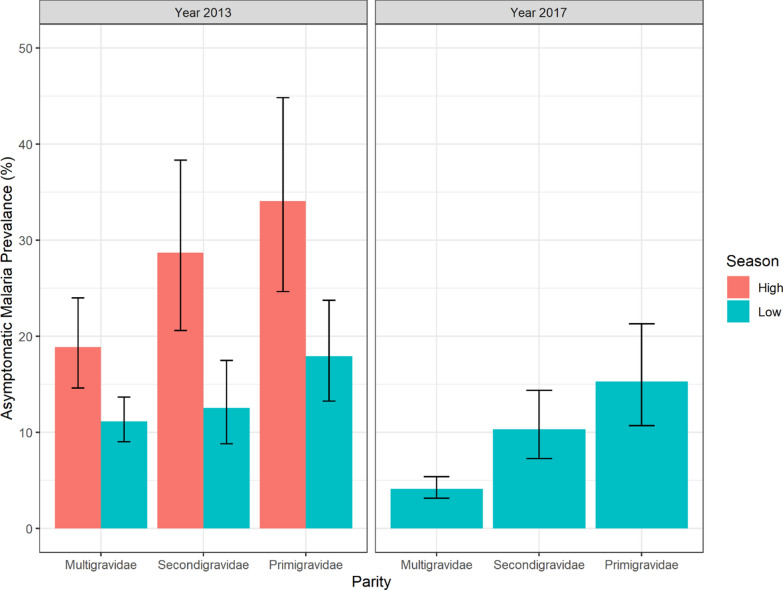
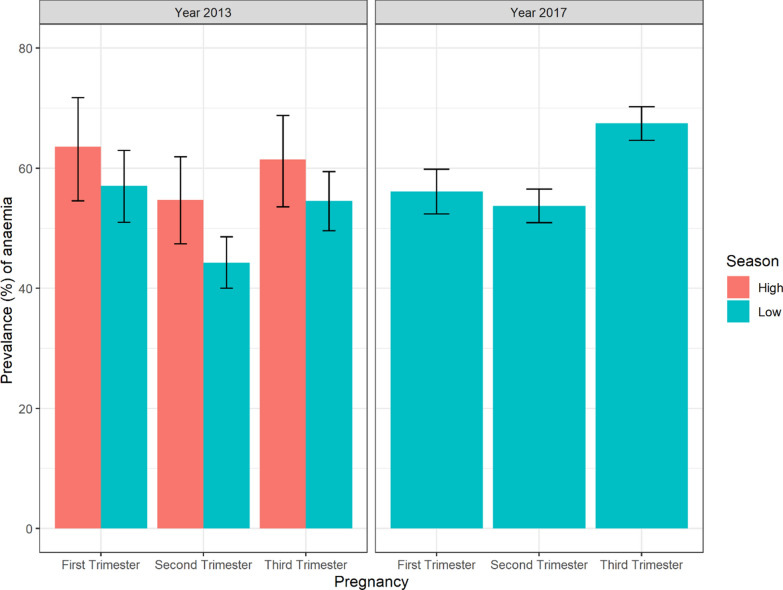
Results: Prevalence of asymptomatic malaria in pregnancy was estimated at 23.9% (95% CI 20.2-28.0) during the high transmission season (October-November) in 2013. During the low transmission season, it was 12.7% (95% CI 10.9-14.7) between December and March in 2013-2014 and halved (6.4%; 95% CI 5.3-7.6) between April and June 2017. Anaemia prevalence was estimated at 59.4% (95% CI 54.8-63.8) during the high transmission season in 2013. During the low transmission season, it was 50.6% (95% CI 47.7-53.4) between December and March 2013-2014 and 65.0% (95% CI 62.8-67.2) between April and June, 2017.
Conclusion: This study revealed that the prevalence of malaria asymptomatic carriage and anaemia among pregnant women at the community level remain high throughout the year. Thus, more efforts are needed to increase prevention measures such as IPTp-SP coverage in order to reduce anaemia and contribute to preventing low birth weight and poor pregnancy outcomes.
Keywords: Asymptomatic carriage; Community; Haemoglobin; Health district; Plasmodium; Pregnant.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- van Geertruyden J-P, Thomas F, Erhart A, D’Alessandro U. The contribution of malaria in pregnancy to perinatal mortality. Am J Trop Med Hyg. 2004;71:35–40. - PubMed
-
- Schwetz J, Peel E. Congenital malaria and placental infections amongst the Negroes of central Africa. Trans R Soc Trop Med Hyg. 1934;28:167–174.
-
- Madanitsa M, Kalilani L, Mwapasa V, van Eijk AM, Khairallah C, Ali D, et al. Scheduled intermittent screening with rapid diagnostic tests and treatment with dihydroartemisinin-piperaquine versus intermittent preventive therapy with sulfadoxine-pyrimethamine for malaria in pregnancy in Malawi: an open-label randomized controlled trial. PLoS Med. 2016;13:e1002124. - PMC - PubMed
-
- Menendez C, Ordi J, Ismail MR, Ventura PJ, Aponte JJ, Kahigwa E, et al. The impact of placental malaria on gestational age and birth weight. J Infect Dis. 2000;181:1740–1745. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
