

Characterization and distribution of medicine vendors in 2 states in Nigeria: implications for scaling health workforce and family planning services
- PMID: 33933081
- PMCID: PMC8088718
- DOI: 10.1186/s12960-021-00602-2
Characterization and distribution of medicine vendors in 2 states in Nigeria: implications for scaling health workforce and family planning services
Abstract
Background: In 2014, Nigeria issued the task-shifting/sharing policy for essential health services, which aimed to fill the human resource gap and improve the delivery of health services across the country. This study focuses on the characteristics, spread, and family planning (FP) stocking practices of medicine vendors in Lagos and Kaduna, assessing the influence of medical training on the provision and stocking of FP services and commodities by vendors.
Methods: We conducted a census of all Patent Medicines stores (PMS) followed up with a facility assessment among 10% of the mapped shops, utilizing an interviewer-administered questionnaire. Bivariate analysis was conducted using the Chi-square test, and multiple logistic regression was used to estimate the adjusted odds ratio (OR) and confidence intervals (CI) for the test of significance in the study.
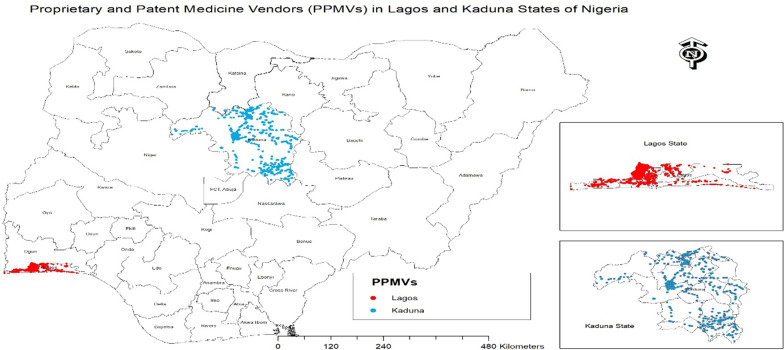
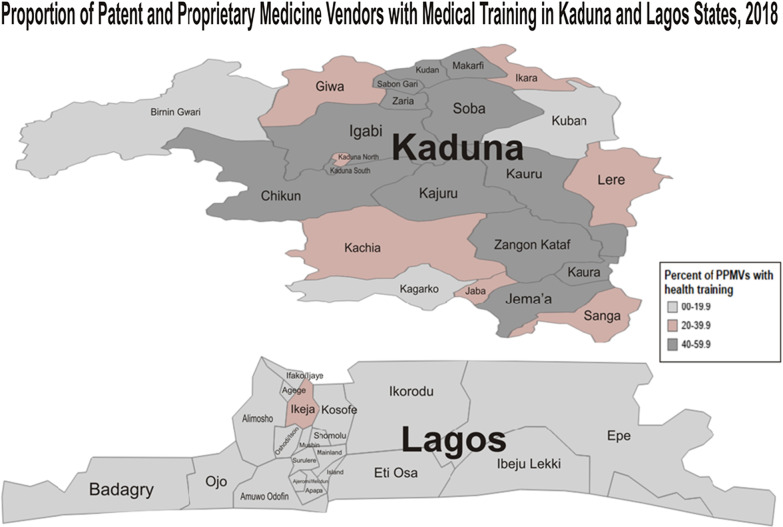
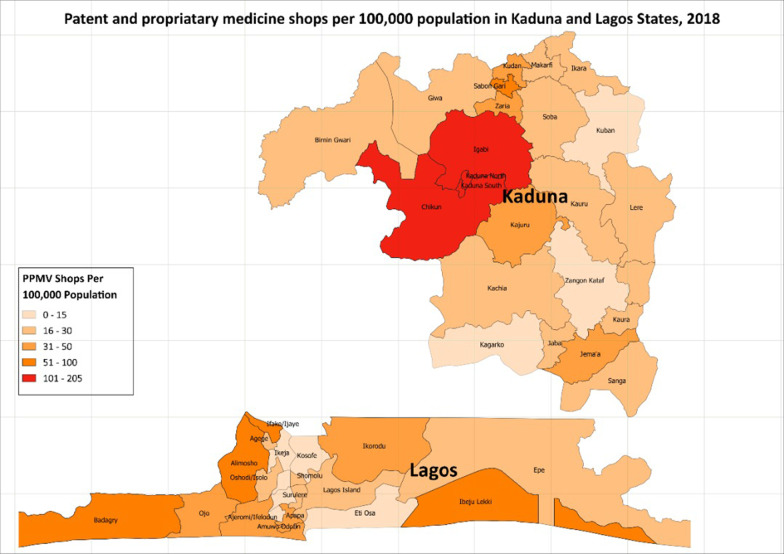
Results: A total of 8318 medicine shops were enumerated (76.2% urban). There were 39 shops per 100,000 population in both states on average. About half (50.9%) were manned by a medicine vendor without assistance, 25.7% claimed to provide FP services to > 2 clients per week, and 11.4% were not registered with the regulatory body or any professional association. Also, 28.2% of vendors reported formal medical training, with 56.3% of these medically trained vendors relatively new in the business, opening within the last 5 years. Vendors utilized open drug markets as the major source of supply for FP products. Medical training significantly increased the stocking of FP products and inhibited utilization of open drug markets.
Conclusion: Patent and Proprietary Medicines Vendor (PPMVs) have continued to grow progressively in the last 5 years, becoming the most proximal health facility for potential clients for different health services (especially FP services) across both Northern and Southern Nigeria, now comprising a considerable mass of medically trained personnel, able to deliver high-quality health services and complement existing healthcare infrastructure, if trained. However, restrictions on services within the PPMV premise and lack of access to quality drugs and commodities have resulted in poor practices among PPMVs. There is therefore a need to identify, train, and provide innovative means of improving access to quality-assured products for this group of health workers.
Keywords: Family planning; Health workers; Medical training; PPMVs; Stocking; Task-shifting.
Conflict of interest statement
The authors declare that they do not have any competing interests. The funders of this study did not have any role in the design, planning, or execution of this work.
Figures
References
-
- World Health Organization . Everybody’s business: strengthening health systems to improve health outcomes: WHO’s framework for action. Geneva: World Health Organization; 2007.
-
- Adebayo O, Labiran A, Emerenini CF, Omoruyi L. Health Workforce for 2016–2030: will Nigeria have enough? Int J Innov Healthc Res. 2016;4(1):9–16.
-
- World Health Organization . The World Health Report 2006—working together for health. Geneva: World Health Organization; 2006. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
