

Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: an individual participant-level data meta-analysis
- PMID: 33933205
- PMCID: PMC8102467
- DOI: 10.1016/S0140-6736(21)00590-0
Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: an individual participant-level data meta-analysis
Erratum in
-
Department of Error.Lancet. 2021 May 22;397(10288):1884. doi: 10.1016/S0140-6736(21)01069-2. Lancet. 2021. PMID: 34022983 Free PMC article. No abstract available.
Abstract
Background: The effects of pharmacological blood pressure lowering at normal or high-normal blood pressure ranges in people with or without pre-existing cardiovascular disease remains uncertain. We analysed individual participant data from randomised trials to investigate the effects of blood pressure lowering treatment on the risk of major cardiovascular events by baseline levels of systolic blood pressure.
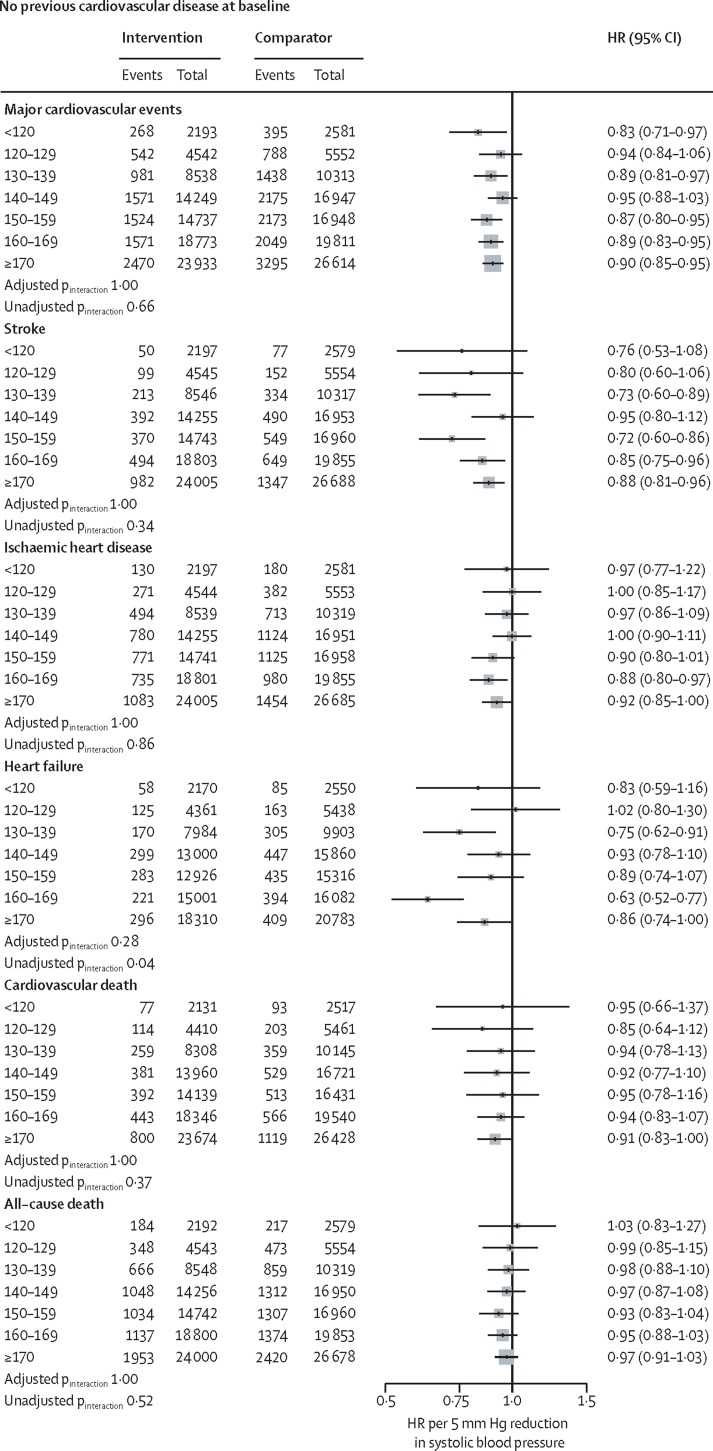
Methods: We did a meta-analysis of individual participant-level data from 48 randomised trials of pharmacological blood pressure lowering medications versus placebo or other classes of blood pressure-lowering medications, or between more versus less intensive treatment regimens, which had at least 1000 persons-years of follow-up in each group. Trials exclusively done with participants with heart failure or short-term interventions in participants with acute myocardial infarction or other acute settings were excluded. Data from 51 studies published between 1972 and 2013 were obtained by the Blood Pressure Lowering Treatment Trialists' Collaboration (Oxford University, Oxford, UK). We pooled the data to investigate the stratified effects of blood pressure-lowering treatment in participants with and without prevalent cardiovascular disease (ie, any reports of stroke, myocardial infarction, or ischaemic heart disease before randomisation), overall and across seven systolic blood pressure categories (ranging from <120 to ≥170 mm Hg). The primary outcome was a major cardiovascular event (defined as a composite of fatal and non-fatal stroke, fatal or non-fatal myocardial infarction or ischaemic heart disease, or heart failure causing death or requiring admission to hospital), analysed as per intention to treat.
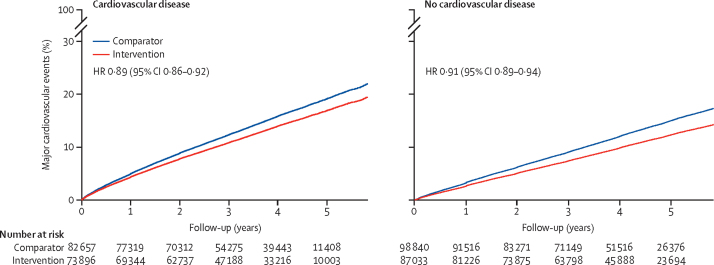
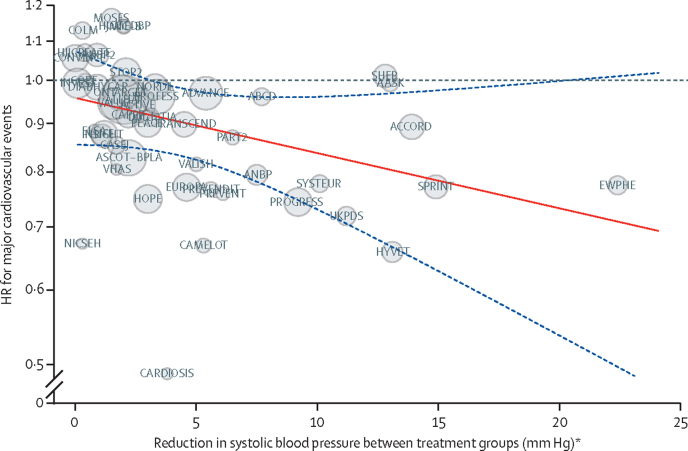
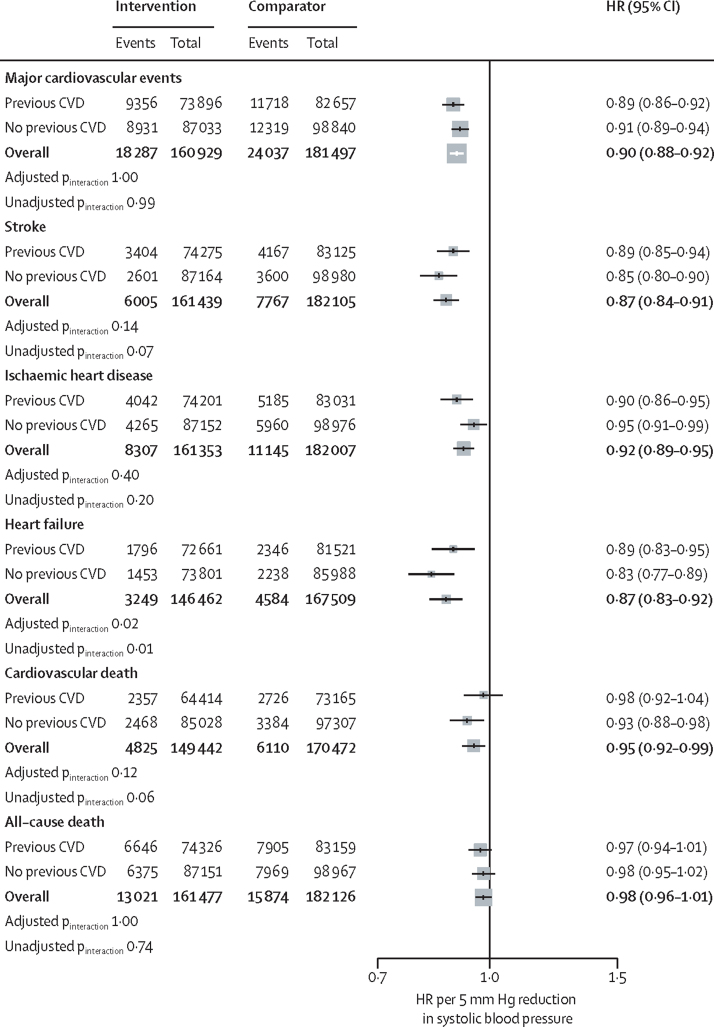
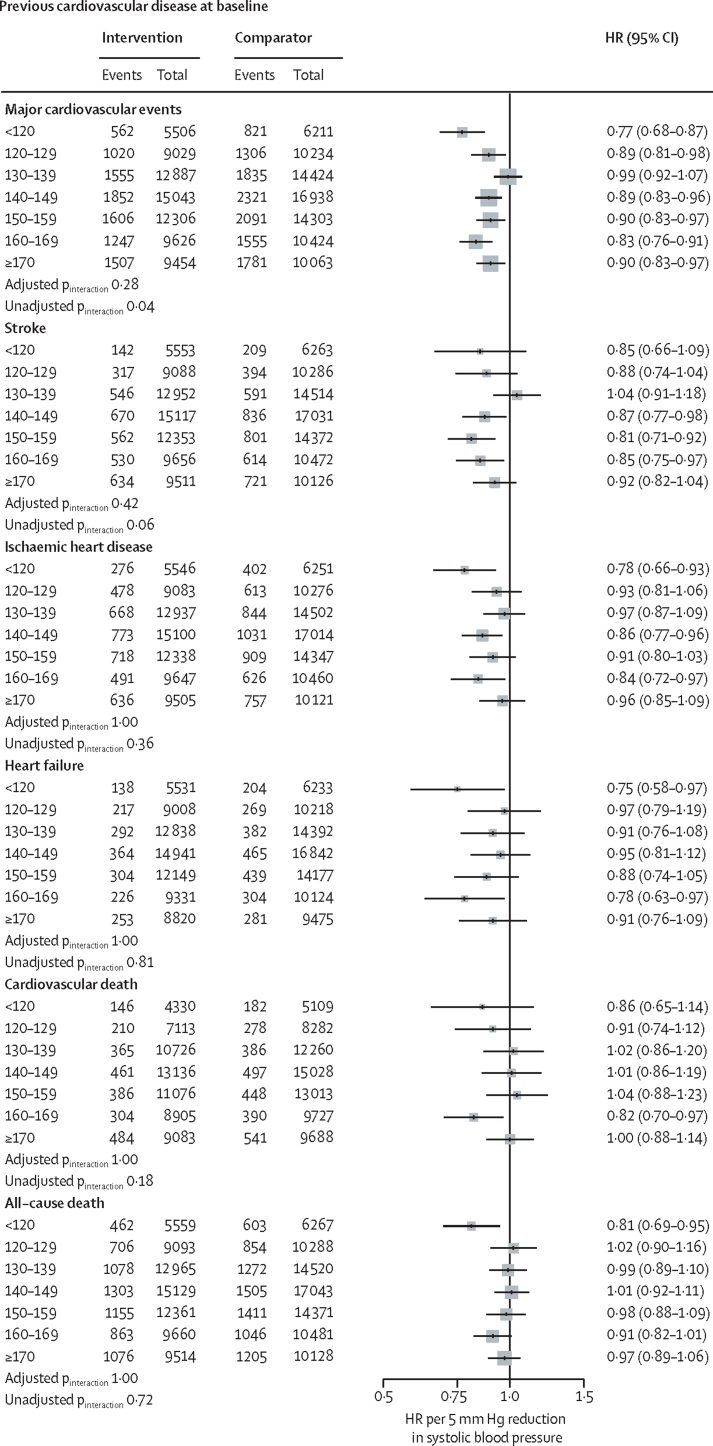
Findings: Data for 344 716 participants from 48 randomised clinical trials were available for this analysis. Pre-randomisation mean systolic/diastolic blood pressures were 146/84 mm Hg in participants with previous cardiovascular disease (n=157 728) and 157/89 mm Hg in participants without previous cardiovascular disease (n=186 988). There was substantial spread in participants' blood pressure at baseline, with 31 239 (19·8%) of participants with previous cardiovascular disease and 14 928 (8·0%) of individuals without previous cardiovascular disease having a systolic blood pressure of less than 130 mm Hg. The relative effects of blood pressure-lowering treatment were proportional to the intensity of systolic blood pressure reduction. After a median 4·15 years' follow-up (Q1-Q3 2·97-4·96), 42 324 participants (12·3%) had at least one major cardiovascular event. In participants without previous cardiovascular disease at baseline, the incidence rate for developing a major cardiovascular event per 1000 person-years was 31·9 (95% CI 31·3-32·5) in the comparator group and 25·9 (25·4-26·4) in the intervention group. In participants with previous cardiovascular disease at baseline, the corresponding rates were 39·7 (95% CI 39·0-40·5) and 36·0 (95% CI 35·3-36·7), in the comparator and intervention groups, respectively. Hazard ratios (HR) associated with a reduction of systolic blood pressure by 5 mm Hg for a major cardiovascular event were 0·91, 95% CI 0·89-0·94 for partipants without previous cardiovascular disease and 0·89, 0·86-0·92, for those with previous cardiovascular disease. In stratified analyses, there was no reliable evidence of heterogeneity of treatment effects on major cardiovascular events by baseline cardiovascular disease status or systolic blood pressure categories.
Interpretation: In this large-scale analysis of randomised trials, a 5 mm Hg reduction of systolic blood pressure reduced the risk of major cardiovascular events by about 10%, irrespective of previous diagnoses of cardiovascular disease, and even at normal or high-normal blood pressure values. These findings suggest that a fixed degree of pharmacological blood pressure lowering is similarly effective for primary and secondary prevention of major cardiovascular disease, even at blood pressure levels currently not considered for treatment. Physicians communicating the indication for blood pressure lowering treatment to their patients should emphasise its importance on reducing cardiovascular risk rather than focusing on blood pressure reduction itself.
Funding: British Heart Foundation, UK National Institute for Health Research, and Oxford Martin School.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests MW reports personal fees from Amgen, Kyowa Kirin, and Freeline. MN and DC report grants from the British Heart Foundation (BHF). KR reports grants from BHF, the UK Research and Innovation Global Challenges Research Fund, Oxford Martin School (University of Oxford, Oxford, UK), and National Institute for Health Research Oxford Biomedical Research Centre (University of Oxford); and personal fees from British Medical Journal Heart and Public Library of Science Medicine. JC reports grants from the National Health and Medical Research Council of Australia. EC, ZB, RR, KKT, CJP, A-CP-G, and BRD declare no competing interests.
Figures
Comment in
-
Decisions about antihypertensive treatment should focus on reducing cardiovascular risk.Lancet. 2021 May 1;397(10285):1598-1599. doi: 10.1016/S0140-6736(21)00877-1. Lancet. 2021. PMID: 33933193 No abstract available.
-
Are blood-pressure targets needed to prevent cardiovascular disease?Nat Rev Cardiol. 2021 Sep;18(9):615-616. doi: 10.1038/s41569-021-00595-4. Nat Rev Cardiol. 2021. PMID: 34230648 No abstract available.
-
The key role of blood pressure lowering in cardiovascular prevention irrespective of baseline blood pressure and risk profile.Eur Heart J. 2021 Jul 31;42(29):2814-2815. doi: 10.1093/eurheartj/ehab320. Eur Heart J. 2021. PMID: 34333600 No abstract available.
-
Blood pressure treatment: how low should you go? - Authors' reply.Lancet. 2021 Nov 6;398(10312):1684-1685. doi: 10.1016/S0140-6736(21)01856-0. Lancet. 2021. PMID: 34742378 No abstract available.
-
Blood pressure treatment: how low should you go?Lancet. 2021 Nov 6;398(10312):1684. doi: 10.1016/S0140-6736(21)01857-2. Lancet. 2021. PMID: 34742379 No abstract available.
-
Frühzeitig fix kombinieren!MMW Fortschr Med. 2021 Dec;163(21-22):82. doi: 10.1007/s15006-021-0607-z. MMW Fortschr Med. 2021. PMID: 34888824 German. No abstract available.
References
-
- Ettehad D, Emdin CA, Kiran A. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016;387:957–967. - PubMed
-
- Williams B, Mancia G, Spiering W. 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J. 2018;39:3021–3104. - PubMed
-
- Whelton PK, Carey RM, Aronow WS. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. J Am Coll Cardiol. 2018;71:e127–e248. - PubMed
-
- UK National Institute for Health and Care Excellence Hypertension in adults: diagnosis and management (NICE guideline 136) 2019. https://www.nice.org.uk/guidance/ng136 - PubMed
-
- New Zealand Ministry of Health Cardiovascular Disease Risk Assessment and Management for Primary Care. Feb 14, 2018. https://www.health.govt.nz/publication/cardiovascular-disease-risk-asses...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
