

Plasma calcitonin gene-related peptide (CGRP) in migraine and endometriosis during the menstrual cycle
- PMID: 33934575
- PMCID: PMC8164854
- DOI: 10.1002/acn3.51360
Plasma calcitonin gene-related peptide (CGRP) in migraine and endometriosis during the menstrual cycle
Abstract
Objective: Migraine, endometriosis, and the comorbidity of both are frequent pain disorders of special relevance for women. The neuropeptide calcitonin gene-related peptide (CGRP) is critically involved in migraine, and circumstantial evidence suggests a role in endometriosis. We assessed CGRP levels at different times of menstrual cycle in four groups: healthy women, women with migraine or endometriosis and with the comorbidity of both.
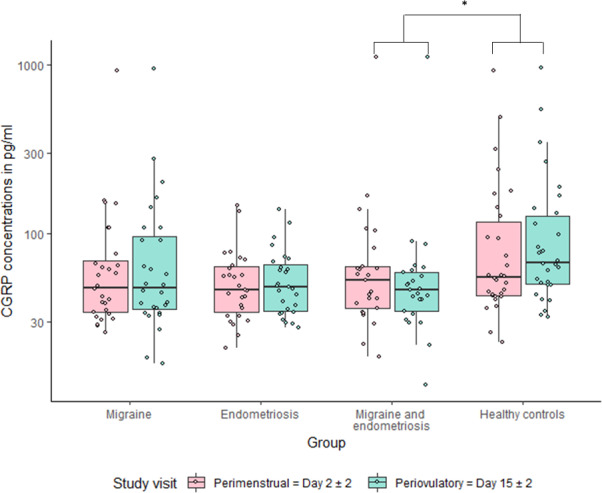
Methods: Women with episodic migraine and women with a histologically confirmed endometriosis were recruited from specialized centers. For CGRP determination with a commercial enzyme immunoassay kit, cubital vein blood samples were collected on menstrual cycle day 2 ± 2 (during menstruation) and on day 15 ± 2 (periovulatory period). The primary endpoint of the study was the absolute difference of CGRP plasma levels between the menstrual and the periovulatory phase of all study groups. Groups were compared using nonparametric test procedures.
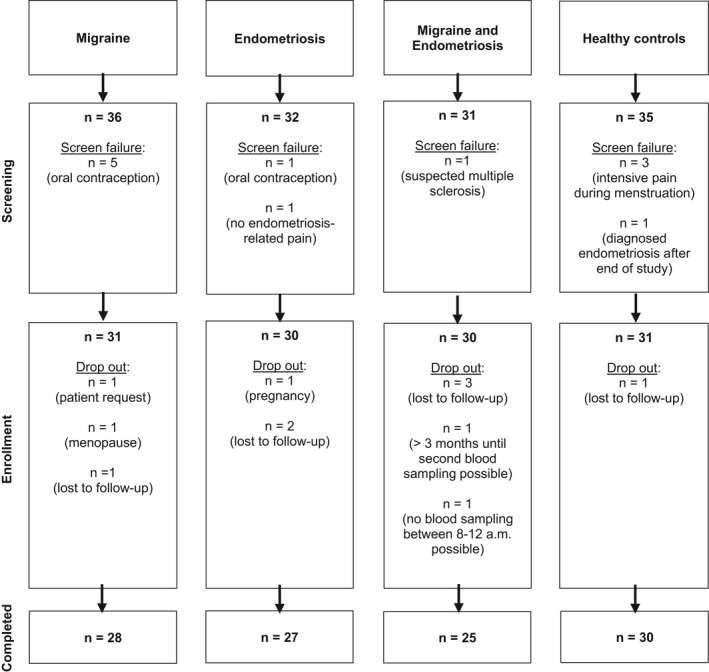
Results: A total of 124 women were included in the study. The change of CGRP plasma levels between menstruation and the periovulatory period was different between groups (p = 0.007). Women with comorbid migraine and endometriosis showed an increase of CGRP in the menstrual phase of +6.32 (interquartile range, IQR -3.64-13.60) compared to the periovulatory time, while healthy controls had a decrease of -10.14 (-22.54-0.91, p = 0.004). CGRP levels were different in the periovulatory phase among groups (p = 0.008), with highest values in healthy controls.
Interpretation: CGRP levels change significantly during the menstrual cycle. Different patterns in women with the comorbidity point to a deviant regulation of CGRP release.
© 2021 The Authors. Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
BR reports grants from Novartis, during the conduct of the study, personal fees from Novartis, Teva, and Allergan, all outside the submitted work. LHO has nothing to disclose. JM reports personal fees from Novartis, outside the submitted work. MDH has nothing to disclose. HK has nothing to disclose. CPN has nothing to disclose. LN reports personal fees from Novartis, Allergan, TEVA, BIAL, Hormosan, and Eli Lilly, all outside the submitted work. ADE has nothing to disclose. JS reports personal fees from Roche, grants and personal fees from Eli Lilly, personal fees from Johnson and Johnson, all outside the submitted work. SM has nothing to disclose. UR reports personal fees from Abbvie, Allergan, Amgen, Eli Lilly, Medscape, Novartis, StreaMedUp, and Teva; institutional fees from Amgen, Eli Lilly, Novartis, Teva, and Alder, and grants from Novartis, all outside the submitted work.
Figures
References
-
- Bulun SE. Endometriosis. N Eng J Med 2009;360(3):268–279. - PubMed
-
- Burch RC, Buse DC, Lipton RB. Migraine: epidemiology, burden, and comorbidity. Neurol Clin 2019;37(4):631–649. - PubMed
-
- Simoens S, Dunselman G, Dirksen C, et al. The burden of endometriosis: costs and quality of life of women with endometriosis and treated in referral centres. Hum Reprod 2012;27(5):1292–1299. - PubMed
-
- Ferrero S, Pretta S, Bertoldi S, et al. Increased frequency of migraine among women with endometriosis. Hum Reprod 2004;19(12):2927–2932. - PubMed
-
- Tietjen GE, Conway A, Utley C, et al. Migraine is associated with menorrhagia and endometriosis. Headache 2006;46(3):422–428. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials