

Bacterial Coinfections in Coronavirus Disease 2019
- PMID: 33934980
- PMCID: PMC8026275
- DOI: 10.1016/j.tim.2021.03.018
Bacterial Coinfections in Coronavirus Disease 2019
Abstract
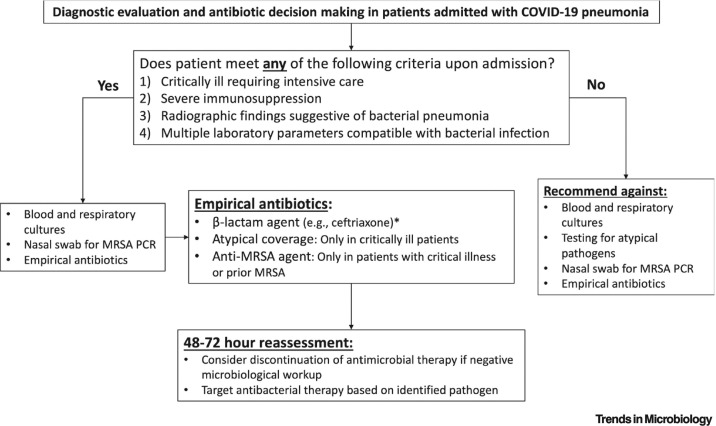
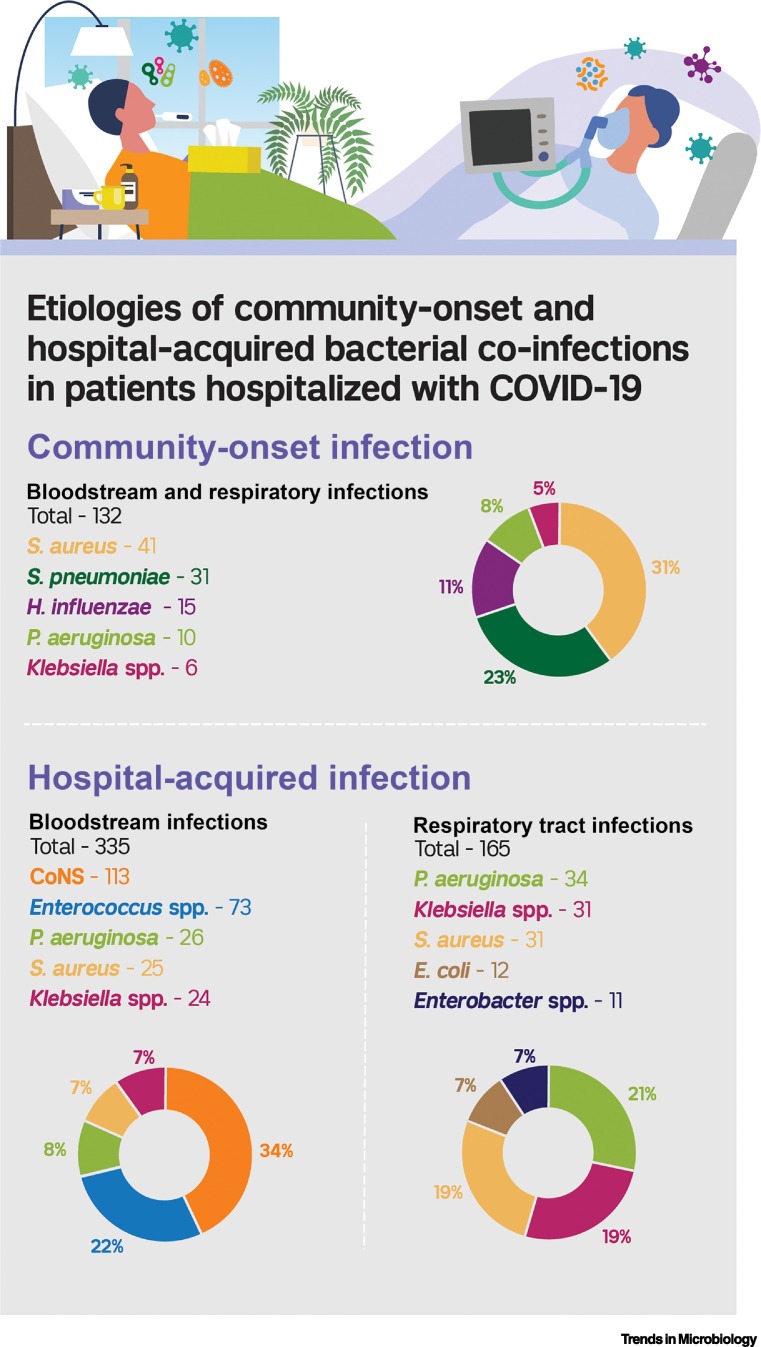
Bacterial coinfections increase the severity of respiratory viral infections and were frequent causes of mortality in influenza pandemics but have not been well characterized in patients with coronavirus disease 2019 (COVID-19). The aim of this review was to identify the frequency and microbial etiologies of bacterial coinfections that are present upon admission to the hospital and that occur during hospitalization for COVID-19. We found that bacterial coinfections were present in <4% of patients upon admission and the yield of routine diagnostic tests for pneumonia was low. When bacterial coinfections did occur, Staphylococcus aureus, Streptococcus pneumoniae, and Haemophilus influenzae were the most common pathogens and atypical bacteria were rare. Although uncommon upon admission, bacterial infections frequently occurred in patients with prolonged hospitalization, and Pseudomonas aeruginosa, Klebsiella spp., and S. aureus were common pathogens. Antibacterial therapy and diagnostic testing for bacterial infections are unnecessary upon admission in most patients hospitalized with COVID-19, but clinicians should be vigilant for nosocomial bacterial infections.
Keywords: bacterial coinfection; coronavirus disease 2019 (COVID-19); hospital-acquired infections; multidrug resistance (MDR); severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of Interests There are no interests to declare.
Figures
References
-
- Martín-Loeches I., et al. Community-acquired respiratory coinfection in critically ill patients with pandemic 2009 influenza A (H1N1) virus. Chest. 2011;139:555–562. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
