

Determination of Ischemia Onset Based on Automatically Generated Spectralis SD-OCT Values in Acute Central Retinal Artery Occlusion
- PMID: 33936808
- PMCID: PMC8060120
- DOI: 10.1155/2021/5527292
Determination of Ischemia Onset Based on Automatically Generated Spectralis SD-OCT Values in Acute Central Retinal Artery Occlusion
Abstract
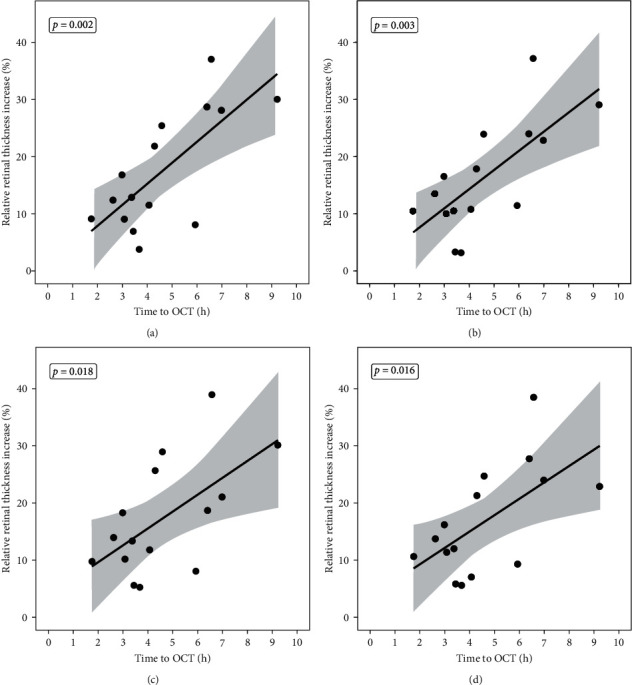
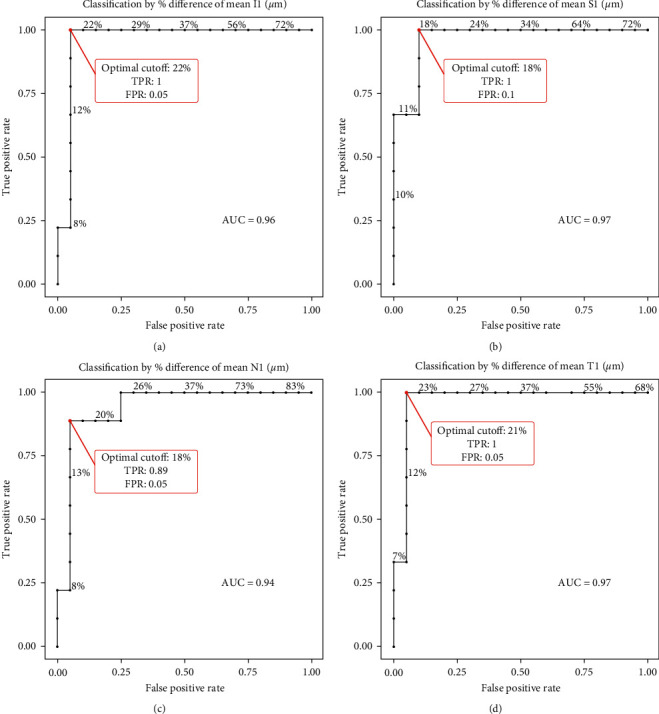
Acute central retinal artery occlusion (CRAO) induces a time-dependent increase in retinal thickness. By manually measuring the relative retinal thickness increase (RRTI) in comparison to the contralateral eye based on optical coherence tomography (OCT), ischemia onset within the past 4.5 hours could be determined with 100% sensitivity and 94.3% specificity. To enable examiner-independent and quicker diagnostics, we analyzed the RRTI using the automatic retinal thickness measurement. In this retrospective study, 28 eyes were evaluated with an acute CRAO (<46 hours). All patients received a Spectralis SD-OCT image of both eyes. The RRTI was calculated for the ETDRS sectors using the Segmentation Module for Single Retinal Layer Analysis. Receiver operating characteristic (ROC) analysis was performed to determine patients ≤4.5 hours by RRTI. In all sectors, time to OCT (TTO) and RRTI correlated positively. The optimal cutoff point to detect CRAOs ≤4.5 hours was between 18.7% nasally and 22.9% RRTI temporally. Sensitivity and specificity varied between the sectors with 90-95% sensitivity and 89-100% specificity. In conclusion, the automatic measurement of RRTI also allows the differentiation of CRAOs within a possible therapeutic time window ≤4.5 hours and CRAOs ≥4.5 hours with a high sensitivity and specificity. Additionally, it offers quicker, easier, and a user-independent assessment of ischemia onset, helping to set a base for establishing automatic indices generated by the OCT machines.
Copyright © 2021 Maria Casagrande et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

References
-
- Wenzel D. A., Kromer R., Poli S., et al. Optical coherence tomography-based determination of ischaemia onset-the temporal dynamics of retinal thickness increase in acute central retinal artery occlusion. Acta Ophthalmology. 2020;99 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
