

Specimen number based diagnostic yields of suspicious axillary lymph nodes in core biopsy in breast cancer: clinical implications from a prospective exploratory study
- PMID: 33936995
- PMCID: PMC8047355
- DOI: 10.21037/qims-20-1030
Specimen number based diagnostic yields of suspicious axillary lymph nodes in core biopsy in breast cancer: clinical implications from a prospective exploratory study
Abstract
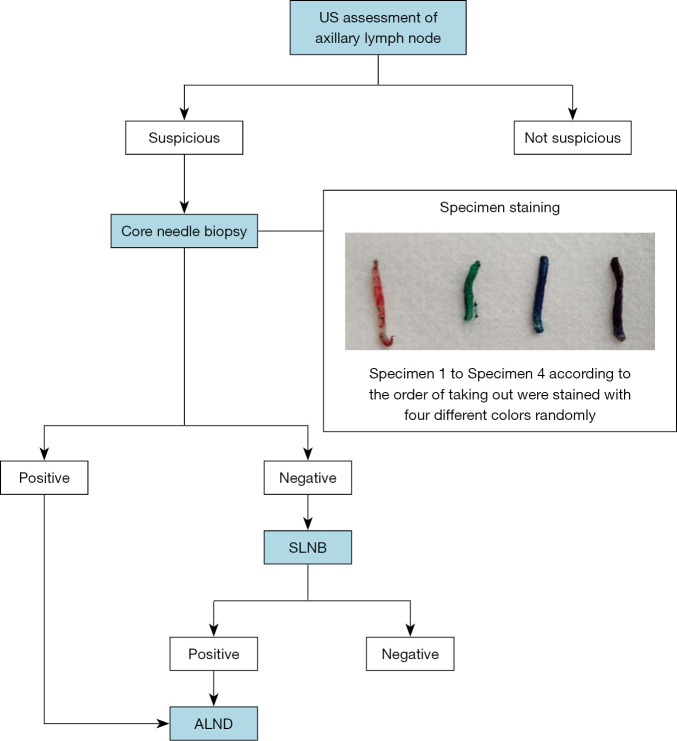
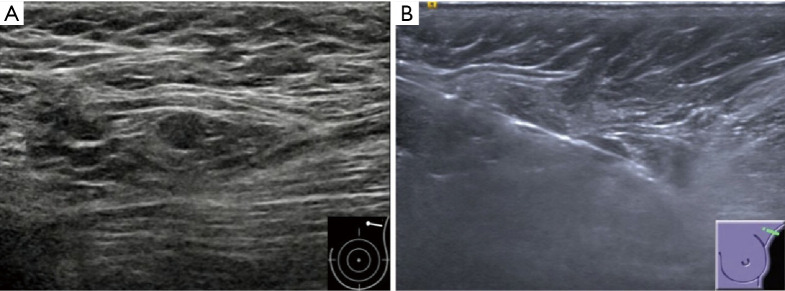
Background: Ultrasound (US)-guided core needle biopsy (CNB) is widely applied in the pathological diagnosis of suspicious axillary lymph nodes (ALNs) in breast cancer. However, the number of specimens removed during biopsy is currently based on the preference of the individual radiologist. This study aims to analyze the specimen number based diagnostic yields of US guided CNB of suspicious ALNs in breast cancer.
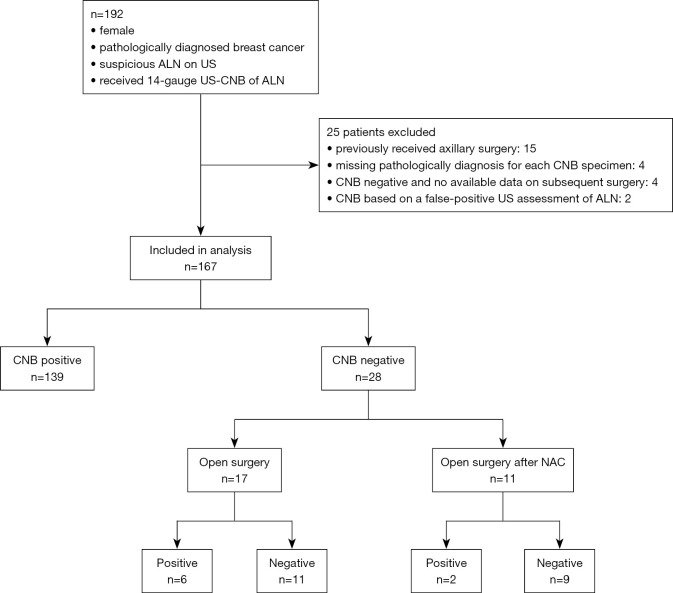
Methods: Core biopsy specimens of suspicious lymph nodes were prospectively obtained from breast cancer patients treated at our hospital between November, 2018, and July, 2019. Four specimens were obtained from each patient and labeled 1-4 in the order they were removed. Each specimen underwent pathological evaluation to determine whether metastasis had occurred. The diagnostic yields of the specimens were calculated and differences in diagnostic accuracy according to the number of specimens were evaluated by McNemar's test.
Results: A total of 167 patients were enrolled, and 139 (83.2%) cases were identified as metastasis by CNB. The diagnostic yields were: 74.2% (specimen 1), 87.8% (specimens 1-2), 91.2% (specimens 1-3), and 94.6% (specimens 1-4). The increases in diagnostic yield from specimen 1 to 1-2 and from specimens 1-2 to 1-4 were significant; however, no significant differences were detected between specimens 1-3 and the first two, or between specimens 1-4 and the first three in this sample size. The lower diagnostic abilities for the first two specimens were associated with shorter long- and short-axis lengths of lymph nodes on US.
Conclusions: Although the second specimen contributed significant diagnostic yield of suspicious axillary lymph nodes in core biopsy in breast cancer, a minimum number cannot be determined by this study. Additional specimens may improve diagnostic yield particularly in patients with small nodes.
Keywords: Breast cancer; axillary lymph node (ALN); core needle biopsy (CNB); specimen; ultrasound (US).
2021 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/qims-20-1030). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Impact of sentinel lymph node biopsy by ultrasound-guided core needle biopsy for patients with suspicious node positive breast cancer.Breast Cancer. 2018 Jan;25(1):86-93. doi: 10.1007/s12282-017-0795-7. Epub 2017 Jul 22. Breast Cancer. 2018. PMID: 28735457
-
Impact of sentinel lymph node biopsy in newly diagnosed invasive breast cancer patients with suspicious node: a comparative accuracy survey of fine-needle aspiration biopsy versus core-needle biopsy.Am J Transl Res. 2018 Jun 15;10(6):1860-1873. eCollection 2018. Am J Transl Res. 2018. PMID: 30018726 Free PMC article.
-
Axillary lymph nodes suspicious for breast cancer metastasis: sampling with US-guided 14-gauge core-needle biopsy--clinical experience in 100 patients.Radiology. 2009 Jan;250(1):41-9. doi: 10.1148/radiol.2493071483. Epub 2008 Oct 27. Radiology. 2009. PMID: 18955508
-
The accuracy of ultrasound-guided fine-needle aspiration and core needle biopsy in diagnosing axillary lymph nodes in women with breast cancer: a systematic review and meta-analysis.Front Oncol. 2023 Jun 21;13:1166035. doi: 10.3389/fonc.2023.1166035. eCollection 2023. Front Oncol. 2023. PMID: 37416528 Free PMC article.
-
Meta-analysis of the diagnostic accuracy of ultrasound-guided fine-needle aspiration and core needle biopsy in diagnosing axillary lymph node metastasis.Br J Surg. 2018 Sep;105(10):1244-1253. doi: 10.1002/bjs.10920. Epub 2018 Jul 4. Br J Surg. 2018. PMID: 29972239
Cited by
-
Ultrasound contrast-enhanced patterns of sentinel lymph nodes: predictive value for nodal status and metastatic burden in early breast cancer.Quant Imaging Med Surg. 2023 Jan 1;13(1):160-170. doi: 10.21037/qims-22-234. Epub 2022 Nov 16. Quant Imaging Med Surg. 2023. PMID: 36620166 Free PMC article.
-
The effectiveness of ultrasound-guided core needle biopsy in detecting lymph node metastases in the axilla in patients with breast cancer: systematic review and meta-analysis.Clinics (Sao Paulo). 2023 May 2;78:100207. doi: 10.1016/j.clinsp.2023.100207. eCollection 2023. Clinics (Sao Paulo). 2023. PMID: 37141768 Free PMC article.
References
-
- Veronesi U, Paganelli G, Viale G, Luini A, Zurrida S, Galimberti V, Intra M, Veronesi P, Robertson C, Maisonneuve P, Renne G, De Cicco C, De Lucia F, Gennari R. A randomized comparison of sentinel-node biopsy with routine axillary dissection in breast cancer. N Engl J Med 2003;349:546-53. 10.1056/NEJMoa012782 - DOI - PubMed
-
- Lyman GH, Giuliano AE, Somerfield MR, Benson AB, III, Bodurka DC, Burstein HJ, Cochran AJ, Cody HS, III, Edge SB, Galper S. American Society of Clinical Oncology guideline recommendations for sentinel lymph node biopsy in early-stage breast cancer. J Clin Oncol 2005;23:7703-20. 10.1200/JCO.2005.08.001 - DOI - PubMed
-
- National comprehensive cancer network. NCCN guidelines. Available online: https://www.nccn.org/professionals/physician_gls/default.aspx
LinkOut - more resources
Full Text Sources
Other Literature Sources