

Home parasternal electromyography tracks patient-reported and physiological measures of recovery from severe COPD exacerbation
- PMID: 33937390
- PMCID: PMC8071974
- DOI: 10.1183/23120541.00709-2020
Home parasternal electromyography tracks patient-reported and physiological measures of recovery from severe COPD exacerbation
Abstract
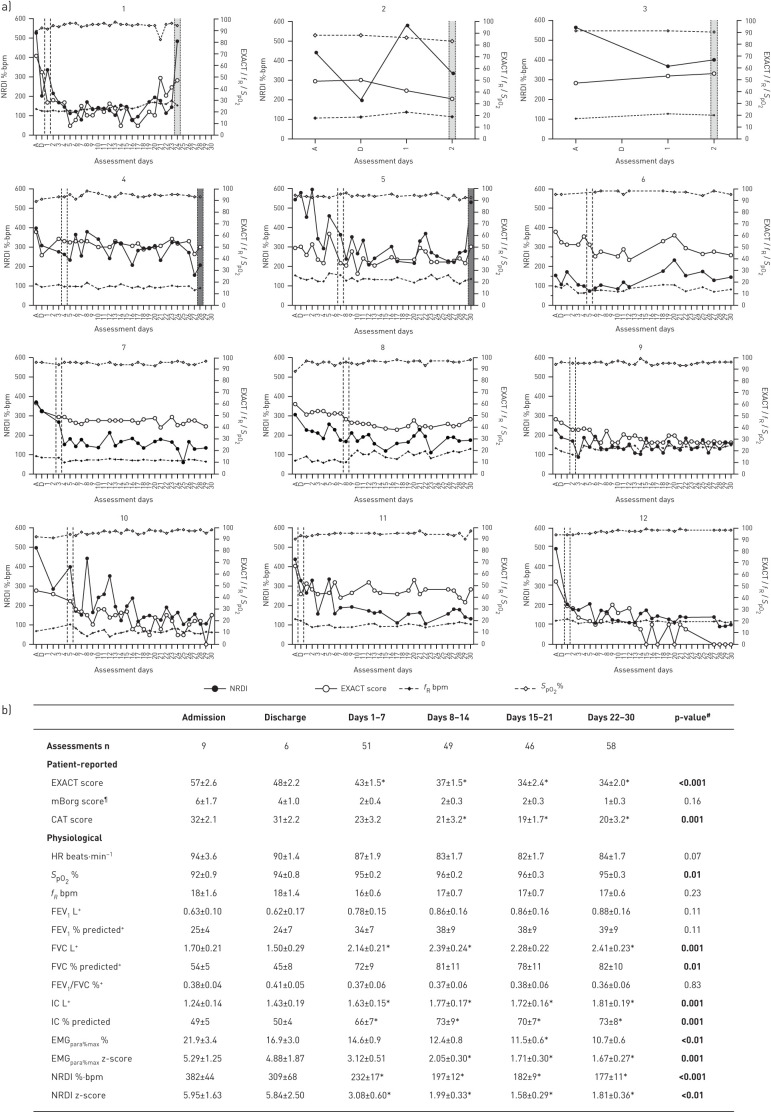
Physiological phenotyping using daily home-based assessments reveals early improvement in load-capacity-drive imbalance following #AECOPD and feasibility of home parasternal electromyography measurement, which tracks symptoms, health status and spirometry https://bit.ly/3o6I0Ty.
Copyright ©The authors 2021.
Conflict of interest statement
Conflict of interest: R.F. D'Cruz reports a Clinical Training Fellowship and Doctoral Research Fellowship (NIHR-INF-0415 and DRF-2018-11-ST2-037) from the National Institute for Health Research during the conduct of the study. Conflict of interest: E-S. Suh reports grants to his institution and fees for CPD approved activity from Philips Research outside the submitted work. Conflict of interest: G. Kaltsakas has nothing to disclose. Conflict of interest: A. Dewar has nothing to disclose. Conflict of interest: N.M. Shah reports grants from Breas, with the funds held and managed by Guy's and St Thomas’ NHS Foundation Trust, outside the submitted work. Conflict of interest: R. Priori is an employee of Philips Research. Conflict of interest: A. Douiri has nothing to disclose. Conflict of interest: L. Rose has nothing to disclose. Conflict of interest: N. Hart reports an unrestricted grant for the OPIP Trial from Philips Respironics, nonfinancial support for development of the Myotrace technology from Philips Respironics RT Meeting (Myotrace), and unrestricted research grants for the HoT-HMV Trial from RESMED and Philips Respironics, outside the submitted work; in addition, he has patents for Myotrace issued in Europe and pending in the USA. His research group has received unrestricted grants (managed by Guy's and St Thomas’ Foundation Trust) from Philips and RESMED. Philips are contributing to the development of the Myotrace technology. Conflict of interest: P.B. Murphy reports grants to his institution and fees for CPD approved activity from Philips, ResMed, F&P and Electromedical, personal fees for an advisory board from Santhera, and grants to his institution from GSK, outside the submitted work.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources