

A systematic review and meta-analysis comparing arthroplasty and internal fixation in the treatment of elderly displaced femoral neck fractures
- PMID: 33937715
- PMCID: PMC8016607
- DOI: 10.1097/OI9.0000000000000087
A systematic review and meta-analysis comparing arthroplasty and internal fixation in the treatment of elderly displaced femoral neck fractures
Abstract
Background: Currently, there are 2 mainstream treatments for displaced femoral neck fracture, including internal fixation and arthroplasty. However, there are still some controversial problems as to which treatment should be primarily chosen.
Methods: The relevant studies comparing arthroplasty with internal fixation were searched in the databases of PubMed, Embase, and Cochrane Library. Finally, 31 relevant randomized controlled trials were included in this meta-analysis. The quality of studies was evaluated and meta-analyses were performed using RevMan 5.3 software. We also assessed the heterogeneity among studies and publication bias via the I-squared index and forest plots.
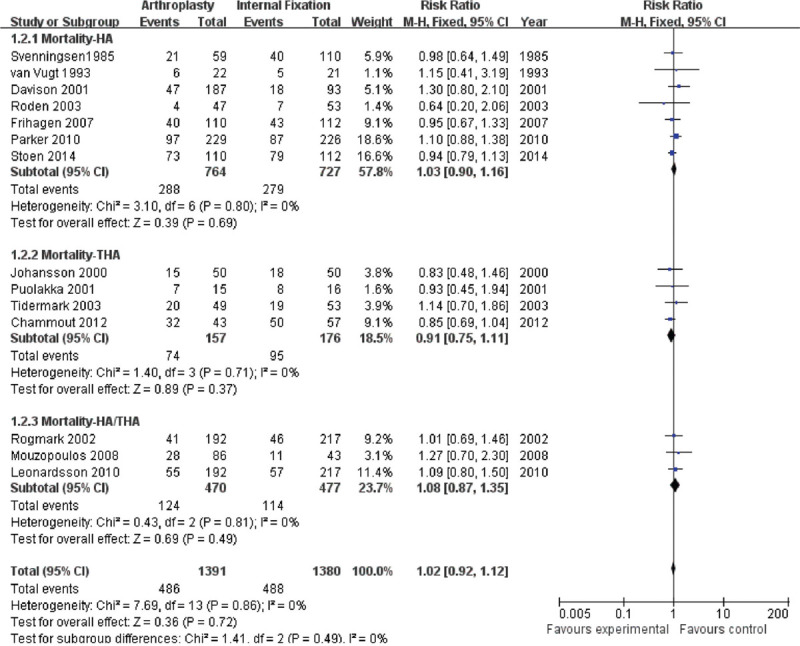
Results: There was no significant difference between arthroplasty and internal fixation groups in patient mortality at both short-term and long-term points. However, patients treated with arthroplasty showed significantly lowered risks of reoperation both at short-term (5.6% vs 31.5%; relative risks (RR) = 0.19; 95% CI, 0.13-0.28; P < .00001) and long-term follow-up (9.5% vs 45.9%; RR = 0.23; 95% CI, 0.17-0.33; P < .00001). Similarly, arthroplasty-treated patients demonstrated a significant decrease in the risk of postoperation complications at short-term (10.3% vs 34.4%; RR = 0.37, 95% CI, 0.24-0.57; P < .00001) and long-term follow-up (11.7% vs 42.5%; RR = 0.30, 95% CI, 0.16-0.57; P < .0002). Besides, patients in the arthroplasty group were associated with better alleviation of pain postoperation (18.3% vs 31.1%; RR = 0.50, 95% CI, 0.33-0.78; P = .002).In trial sequence analyses, all cumulative Z curves except that of mortality crossed the trial sequential monitoring boundaries and conventional boundaries, and required information size has been reached.
Conclusions: Arthroplasty leads to a lower rate of reoperation, a reduced risk of complications, and a better alleviation of postoperation pain both at short-term and long-term follow-up. Most importantly, and according to trial sequence analyses, more than enough evidence has been achieved that arthroplasty does show better outcomes than internal fixation in terms of reoperation rate, complications, and postoperation pain.
Level of evidence: Therapeutic Level I. See Instructions for Authors for a complete description of levels of evidence.
Keywords: arthroplasty; femoral neck fracture; internal fixation.
Copyright © 2020 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Orthopaedic Trauma Association.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures








References
-
- Johnell O, Kanis JA. An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. Osteoporos Int. 2004;11:897–902. - PubMed
-
- Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;12:1726–1733. - PubMed
-
- Cummings SR, Melton LJ. Epidemiology and outcomes of osteoporotic fractures. Lancet. 2002;359:1761–1767. - PubMed
-
- van Balen R, Steyerberg EW, Polder JJ, et al. Hip fracture in elderly patients: outcomes for function, quality of life, and type of residence. Clin Orthop Relat Res. 2001;390:232–243. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials