

Use of regional analgesia and risk of delirium in older adults with multiple rib fractures: An Eastern Association for the Surgery of Trauma multicenter study
- PMID: 33938510
- PMCID: PMC9704032
- DOI: 10.1097/TA.0000000000003258
Use of regional analgesia and risk of delirium in older adults with multiple rib fractures: An Eastern Association for the Surgery of Trauma multicenter study
Abstract
Background: Single-center data demonstrates that regional analgesia (RA) techniques are associated with reduced risk of delirium in older patients with multiple rib fractures. We hypothesized that a similar effect between RA and delirium would be identified in a larger cohort of patients from multiple level I trauma centers.
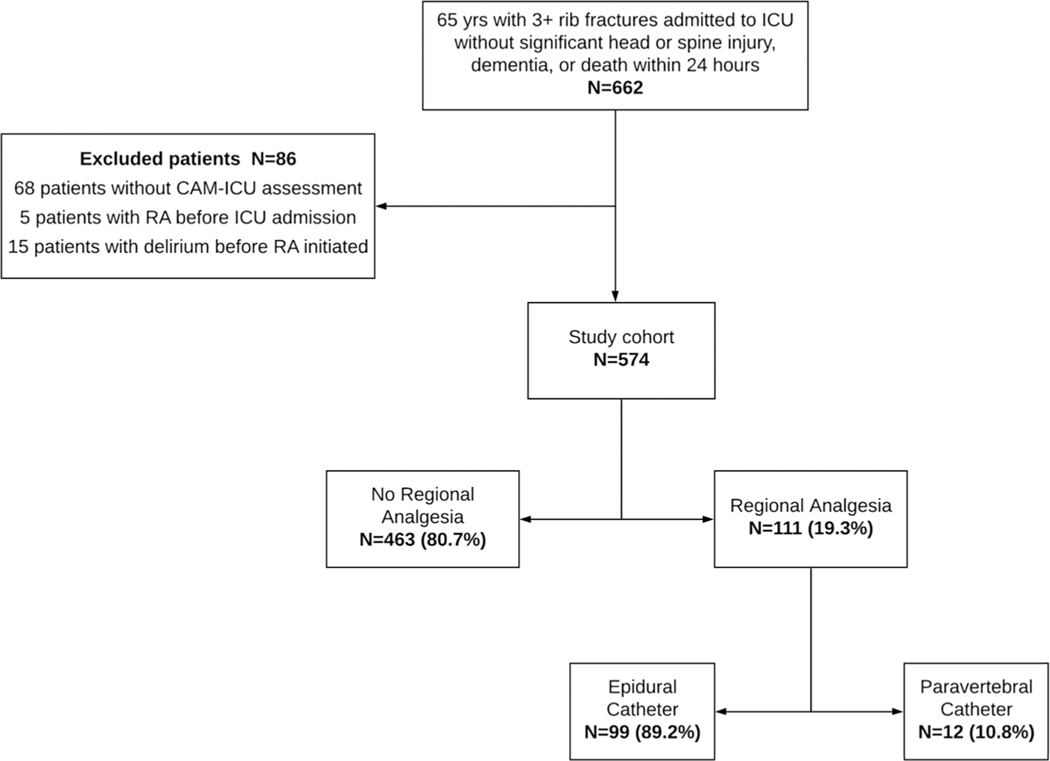
Methods: Retrospective data from seven level I trauma centers were collected for intensive care unit (ICU) patients 65 years or older with ≥3 rib fractures from January 2012 to December 2016. Those with a head and/or spine injury Abbreviated Injury Scale (AIS) score of ≥ 3 or a history of dementia were excluded. Delirium was defined as one positive Confusion Assessment Method for the Intensive Care Unit score in the first 7 days of ICU care. Poisson regression with robust standard errors was used to determine the association of RA (thoracic epidural or paravertebral catheter) with delirium incidence.
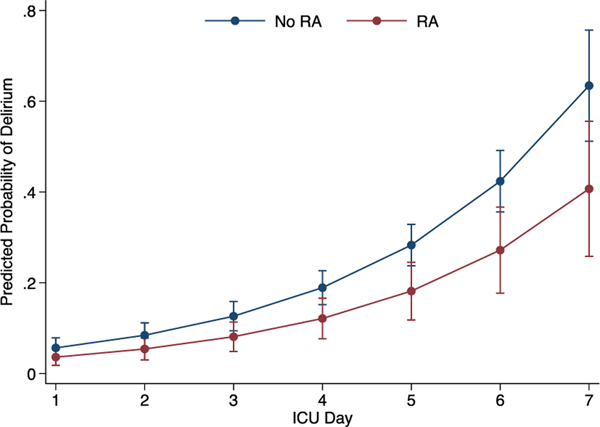
Results: Data of 574 patients with a median age of 75 years (interquartile range [IQR], 69-83), Injury Severity Score of 14 (IQR, 11-18), and ICU length of stay of 3 days (IQR, 2-6 days) were analyzed. Among the patients, 38.9% were women, 15.3% were non-White, and 31.4% required a chest tube. Regional analgesia was used in 19.3% patients. Patient characteristics did not differ by RA use; however, patients with RA had more severe chest injury (chest AIS, flail segment, hemopneumothorax, thoracostomy tube). In univariate analysis, there was no difference in the likelihood of delirium between the RA and no RA groups (18.9% vs. 23.8% p = 0.28). After adjusting for age, sex, Injury Severity Score, maximum chest AIS, thoracostomy tube, ICU length of stay, and trauma center, RA was associated with reduced risk of delirium (incident rate ratio [IRR], 0.65; 95% confidence interval [CI], 0.44-0.94) but not with in-hospital mortality (IRR, 0.42; 95% CI, 0.14-1.26) or respiratory complications (IRR, 0.70; 95% CI, 0.42-1.16).
Conclusion: In this multicenter cohort of injured older adults with multiple rib fractures, RA use was associated with a 35% lower risk of delirium. Further studies are needed to standardize protocols for optimal pain management and prevention of delirium in older adults with severe thoracic injury.
Level of evidence: Therapeutic, level IV; Epidemiologic, level III.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
DISCLOSURE
The authors declare no conflicts of interest.
Figures
Similar articles
-
Decreased Risk of Delirium With Use of Regional Analgesia in Geriatric Trauma Patients With Multiple Rib Fractures.Ann Surg. 2018 Sep;268(3):534-540. doi: 10.1097/SLA.0000000000002929. Ann Surg. 2018. PMID: 30048325
-
Association Between Adherence to Evidence-Based Practices for Treatment of Patients With Traumatic Rib Fractures and Mortality Rates Among US Trauma Centers.JAMA Netw Open. 2020 Mar 2;3(3):e201316. doi: 10.1001/jamanetworkopen.2020.1316. JAMA Netw Open. 2020. PMID: 32215632 Free PMC article.
-
Intercostal liposomal bupivacaine injection for rib fractures: A prospective randomized controlled trial.J Trauma Acute Care Surg. 2022 Feb 1;92(2):266-276. doi: 10.1097/TA.0000000000003462. J Trauma Acute Care Surg. 2022. PMID: 34789700
-
Non-surgical management and analgesia strategies for older adults with multiple rib fractures: A systematic review, meta-analysis, and joint practice management guideline from the Eastern Association for the Surgery of Trauma and the Chest Wall Injury Society.J Trauma Acute Care Surg. 2023 Mar 1;94(3):398-407. doi: 10.1097/TA.0000000000003830. Epub 2022 Nov 15. J Trauma Acute Care Surg. 2023. PMID: 36730672
-
Lessons from a large trauma center: impact of blunt chest trauma in polytrauma patients-still a relevant problem?Scand J Trauma Resusc Emerg Med. 2017 Apr 20;25(1):42. doi: 10.1186/s13049-017-0384-y. Scand J Trauma Resusc Emerg Med. 2017. PMID: 28427480 Free PMC article. Review.
Cited by
-
It takes a village and a multimodal toolbox: pain control after multiple rib fractures.Trauma Surg Acute Care Open. 2024 Jun 13;9(1):e001478. doi: 10.1136/tsaco-2024-001478. eCollection 2024. Trauma Surg Acute Care Open. 2024. PMID: 38881828 Free PMC article. No abstract available.
-
Ultrasound-guided Percutaneous Cryoneurolysis for the Treatment of Pain after Traumatic Rib Fracture: A Randomized, Active-controlled, Participant- and Observer-masked Study.Anesthesiology. 2025 Mar 1;142(3):532-545. doi: 10.1097/ALN.0000000000005328. Epub 2024 Dec 19. Anesthesiology. 2025. PMID: 39723886 Free PMC article. Clinical Trial.
-
Flail chest injury-changing management and outcomes.Eur J Trauma Emerg Surg. 2023 Apr;49(2):1047-1055. doi: 10.1007/s00068-022-02152-1. Epub 2022 Nov 1. Eur J Trauma Emerg Surg. 2023. PMID: 36318281 Free PMC article.
-
Prevalence of Psychiatric Morbidity Among the Elderly Patients Presenting to Emergency Trauma Setting: An Exploratory Study.Indian J Orthop. 2025 Mar 4;59(5):635-643. doi: 10.1007/s43465-025-01342-4. eCollection 2025 May. Indian J Orthop. 2025. PMID: 40321478
-
Analgesia for rib fractures: a narrative review.Can J Anaesth. 2024 Apr;71(4):535-547. doi: 10.1007/s12630-024-02725-1. Epub 2024 Mar 8. Can J Anaesth. 2024. PMID: 38459368 Review. English.
References
-
- Bryczkowski SB, Lopreiato MC, Yonclas PP, Sacca JJ, Mosenthal AC. Risk factors for delirium in older trauma patients admitted to the surgical intensive care unit. J Trauma Acute Care Surg. 2014;77(6):944–951. - PubMed
-
- Bryant EA, Tulebaev S, Castillo-Angeles M, Moberg E, Senglaub SS, O’Mara L, McDonald M, Salim A, Cooper Z. Frailty identification and care pathway: an interdisciplinary approach to care for older trauma patients. J Am Coll Surg. 2019;228(6):852–9.e1. - PubMed
-
- Ely EW, Shintani A, Truman B, Speroff T, Gordon SM, Harrell FE Jr., Inouye SK, Bernard GR, Dittus RS. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004;291(14):1753–1762. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
