

Identifying High-Risk Subphenotypes and Associated Harms From Delayed Antibiotic Orders and Delivery
- PMID: 33938715
- PMCID: PMC8448901
- DOI: 10.1097/CCM.0000000000005054
Identifying High-Risk Subphenotypes and Associated Harms From Delayed Antibiotic Orders and Delivery
Abstract
Objectives: Early antibiotic administration is a central component of sepsis guidelines, and delays may increase mortality. However, prior studies have examined the delay to first antibiotic administration as a single time period even though it contains two distinct processes: antibiotic ordering and antibiotic delivery, which can each be targeted for improvement through different interventions. The objective of this study was to characterize and compare patients who experienced order or delivery delays, investigate the association of each delay type with mortality, and identify novel patient subphenotypes with elevated risk of harm from delays.
Design: Retrospective analysis of multicenter inpatient data.
Setting: Two tertiary care medical centers (2008-2018, 2006-2017) and four community-based hospitals (2008-2017).
Patients: All patients admitted through the emergency department who met clinical criteria for infection.
Interventions: None.
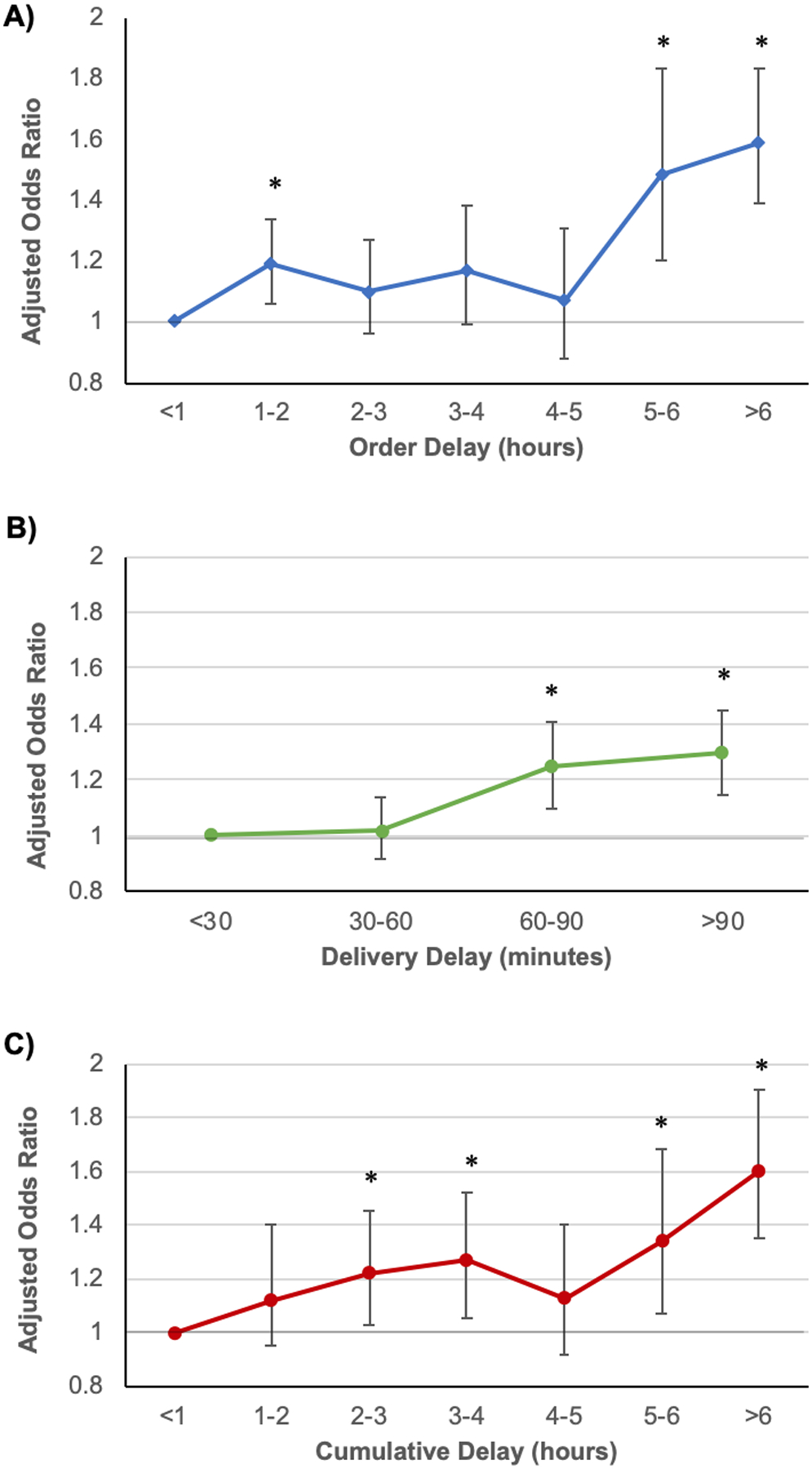
Measurements and main results: Patient demographics, vitals, laboratory values, medication order and administration times, and in-hospital survival data were obtained from the electronic health record. Order and delivery delays were calculated for each admission. Adjusted logistic regression models were used to examine the relationship between each delay and in-hospital mortality. Causal forests, a machine learning method, was used to identify a high-risk subgroup. A total of 60,817 admissions were included, and delays occurred in 58% of patients. Each additional hour of order delay (odds ratio, 1.04; 95% CI, 1.03-1.05) and delivery delay (odds ratio, 1.05; 95% CI, 1.02-1.08) was associated with increased mortality. A patient subgroup identified by causal forests with higher comorbidity burden, greater organ dysfunction, and abnormal initial lactate measurements had a higher risk of death associated with delays (odds ratio, 1.07; 95% CI, 1.06-1.09 vs odds ratio, 1.02; 95% CI, 1.01-1.03).
Conclusions: Delays in antibiotic ordering and drug delivery are both associated with a similar increase in mortality. A distinct subgroup of high-risk patients exist who could be targeted for more timely therapy.
Copyright © 2021 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved.
Conflict of interest statement
Drs. Han’s, Spicer’s, and Churpek’s institutions received funding from the National Institutes of Health (NIH)/National Heart, Blood, and Lung Institute grant T32 HL007605. Dr. Han is supported by the NIH grant T32 HL007605. Drs. Spicer, Afshar, and Churpek received support for article research from the NIH. Dr. Laiteerapong is supported by the NIH grants R01 MD013420, U18 HS026151, and R18 HS027910. Dr. Afshar is supported by the NIH grants K23 AA024503 and R01 DA051464. Dr. Kashiouris received funding from Xelia Pharmaceuticals. Dr. Churpek is supported by the NIH grant R01 GM123193. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures

Comment in
-
Antibiotic Administration and Timing: Risks, Delay, Zombies.Crit Care Med. 2021 Oct 1;49(10):1818-1821. doi: 10.1097/CCM.0000000000005151. Crit Care Med. 2021. PMID: 34529613 No abstract available.
References
-
- Liu V, Escobar GJ, Greene JD, et al.: Hospital Deaths in Patients With Sepsis From 2 Independent Cohorts. JAMA. 2014;312(1):90–92. - PubMed
-
- Hospital Inpatient Specifications Manuals. AccessedSeptember 3, 2020. https://www.qualitynet.org/inpatient/specifications-manuals
-
- Rhodes A, Evans LE, Alhazzani W, et al.: Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Crit Care Med. 2017;45(3):486–552. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
