

Association Between Intracerebral Hemorrhage and Subsequent Arterial Ischemic Events in Participants From 4 Population-Based Cohort Studies
- PMID: 33938907
- PMCID: PMC8094038
- DOI: 10.1001/jamaneurol.2021.0925
Association Between Intracerebral Hemorrhage and Subsequent Arterial Ischemic Events in Participants From 4 Population-Based Cohort Studies
Abstract
Importance: Intracerebral hemorrhage and arterial ischemic disease share risk factors, to our knowledge, but the association between the 2 conditions remains unknown.
Objective: To evaluate whether intracerebral hemorrhage was associated with an increased risk of incident ischemic stroke and myocardial infarction.
Design, setting, and participants: An analysis was conducted of pooled longitudinal participant-level data from 4 population-based cohort studies in the United States: the Atherosclerosis Risk in Communities (ARIC) study, the Cardiovascular Health Study (CHS), the Northern Manhattan Study (NOMAS), and the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study. Patients were enrolled from 1987 to 2007, and the last available follow-up was December 31, 2018. Data were analyzed from September 1, 2019, to March 31, 2020.
Exposure: Intracerebral hemorrhage, as assessed by an adjudication committee based on predefined clinical and radiologic criteria.
Main outcomes and measures: The primary outcome was an arterial ischemic event, defined as a composite of ischemic stroke or myocardial infarction, centrally adjudicated within each study. Secondary outcomes were ischemic stroke and myocardial infarction. Participants with prevalent intracerebral hemorrhage, ischemic stroke, or myocardial infarction at their baseline study visit were excluded. Cox proportional hazards regression was used to examine the association between intracerebral hemorrhage and subsequent arterial ischemic events after adjustment for baseline age, sex, race/ethnicity, vascular comorbidities, and antithrombotic medications.
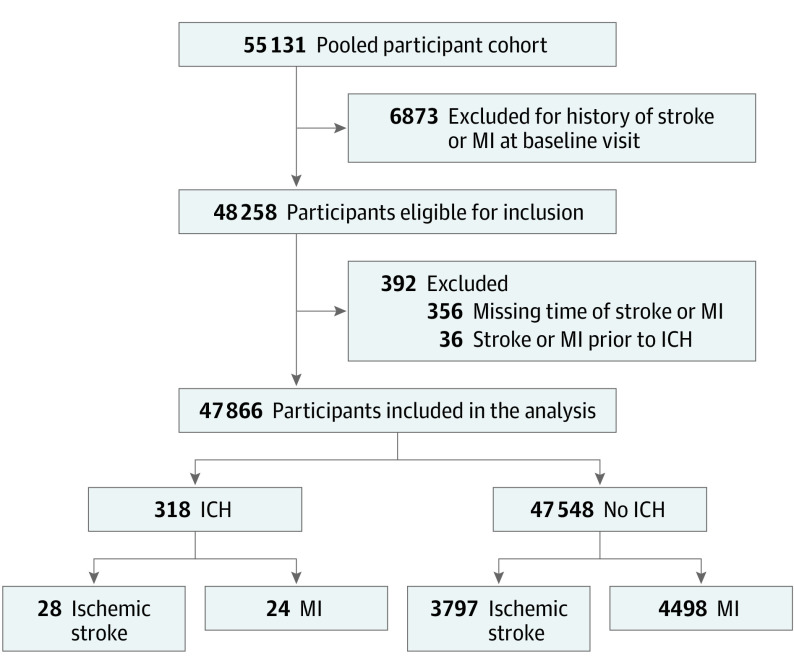
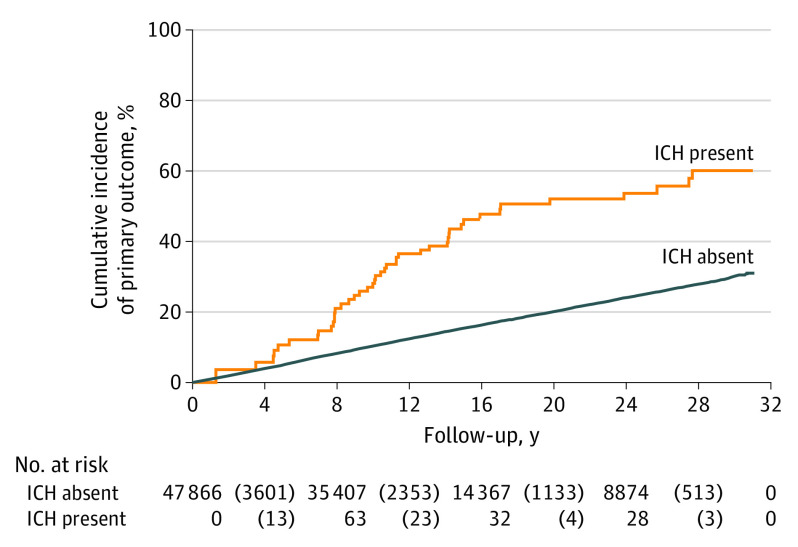
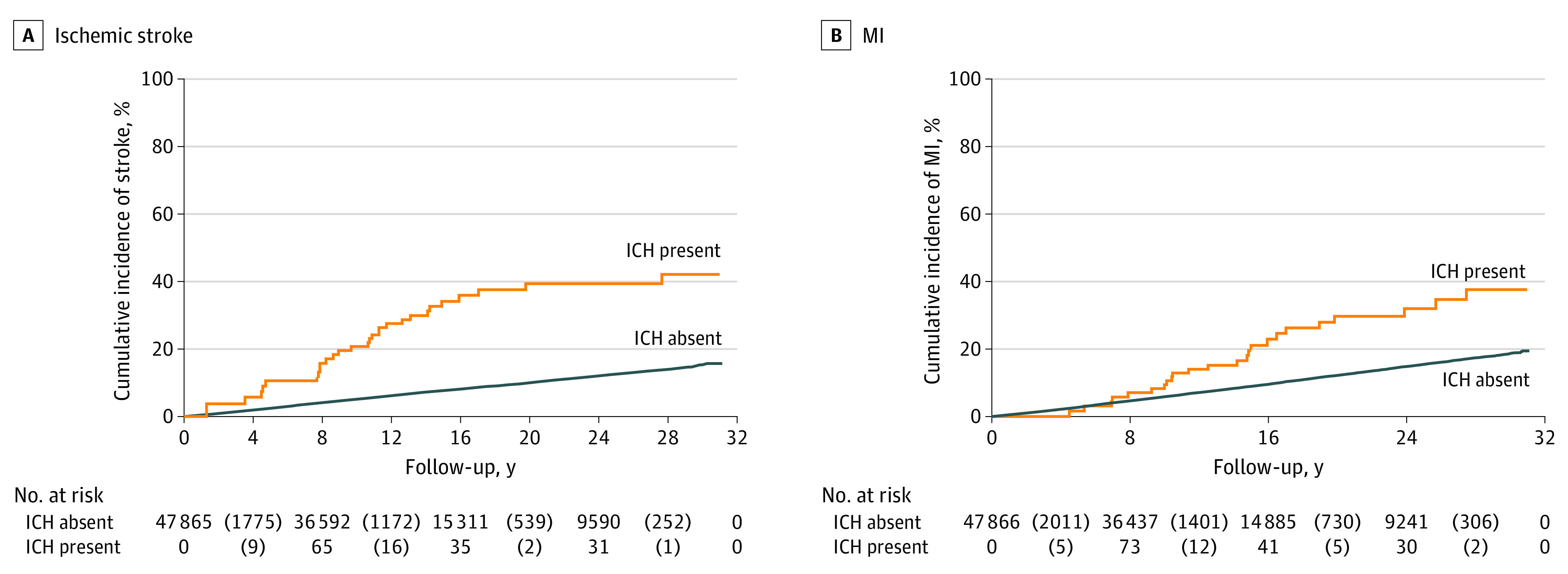
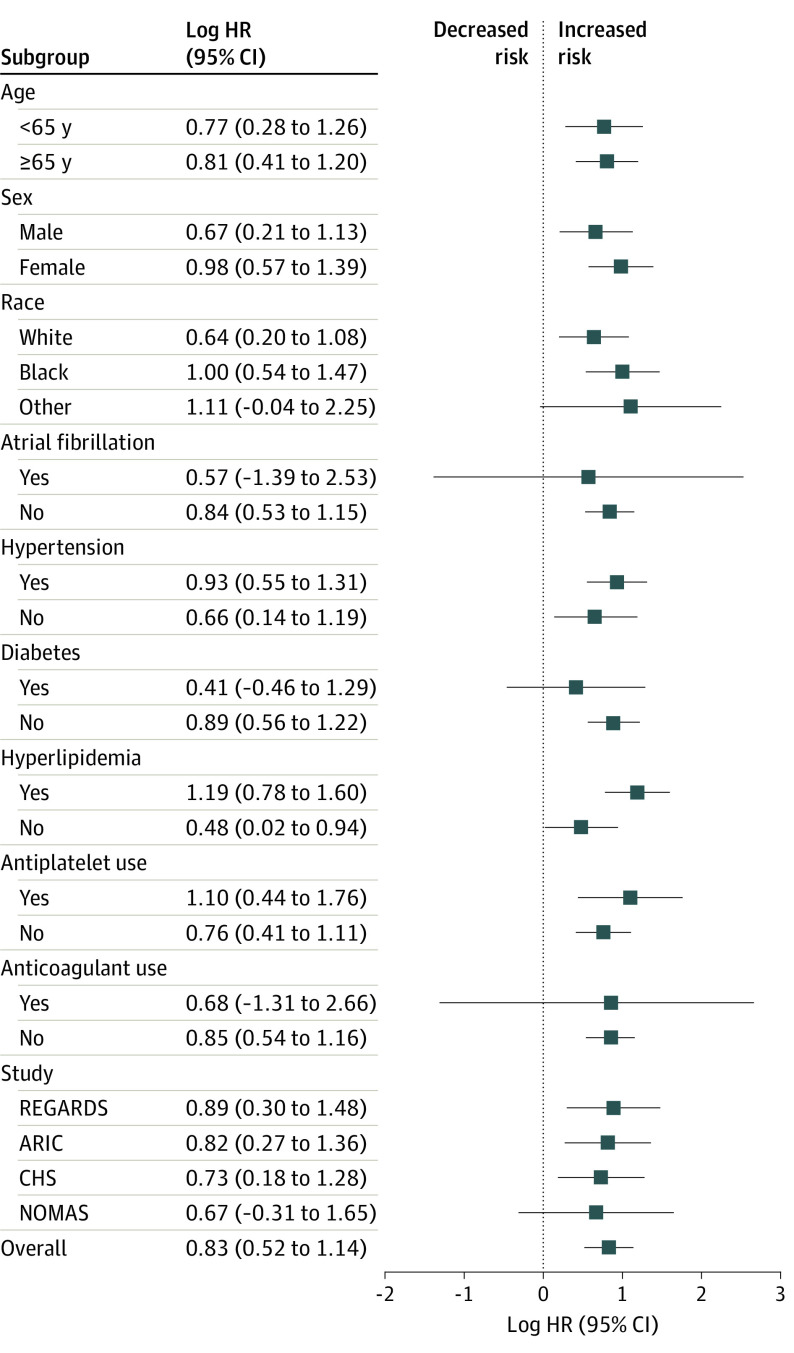
Results: Of 55 131 participants, 47 866 (27 639 women [57.7%]; mean [SD] age, 62.2 [10.2] years) were eligible for analysis. During a median follow-up of 12.7 years (interquartile range, 7.7-19.5 years), there were 318 intracerebral hemorrhages and 7648 arterial ischemic events. The incidence of an arterial ischemic event was 3.6 events per 100 person-years (95% CI, 2.7-5.0 events per 100 person-years) after intracerebral hemorrhage vs 1.1 events per 100 person-years (95% CI, 1.1-1.2 events per 100 person-years) among those without intracerebral hemorrhage. In adjusted models, intracerebral hemorrhage was associated with arterial ischemic events (hazard ratio [HR], 2.3; 95% CI, 1.7-3.1), ischemic stroke (HR, 3.1; 95% CI, 2.1-4.5), and myocardial infarction (HR, 1.9; 95% CI, 1.2-2.9). In sensitivity analyses, intracerebral hemorrhage was associated with arterial ischemic events when updating covariates in a time-varying manner (HR, 2.2; 95% CI, 1.6-3.0); when using incidence density matching (odds ratio, 2.3; 95% CI, 1.3-4.2); when including participants with prevalent intracerebral hemorrhage, ischemic stroke, or myocardial infarction (HR, 2.2; 95% CI, 1.6-2.9); and when using death as a competing risk (subdistribution HR, 1.6; 95% CI, 1.1-2.1).
Conclusions and relevance: This study found that intracerebral hemorrhage was associated with an increased risk of ischemic stroke and myocardial infarction. These findings suggest that intracerebral hemorrhage may be a novel risk marker for arterial ischemic events.
Conflict of interest statement
Figures
Comment in
-
Ischemic Events After Intracerebral Hemorrhage: A New Target for Secondary Prevention.JAMA Neurol. 2021 Jul 1;78(7):795-797. doi: 10.1001/jamaneurol.2021.0772. JAMA Neurol. 2021. PMID: 33938906 No abstract available.
References
-
- Mozaffarian D, Benjamin EJ, Go AS, et al. ; Writing Group Members; American Heart Association Statistics Committee; Stroke Statistics Subcommittee . Heart disease and stroke statistics—2016 update: a report from the American Heart Association. Circulation. 2016;133(4):e38-e360. doi:10.1161/CIR.0000000000000350 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
