

Trends in Patient Characteristics and COVID-19 In-Hospital Mortality in the United States During the COVID-19 Pandemic
- PMID: 33938933
- PMCID: PMC8094014
- DOI: 10.1001/jamanetworkopen.2021.8828
Trends in Patient Characteristics and COVID-19 In-Hospital Mortality in the United States During the COVID-19 Pandemic
Abstract
Importance: In-hospital mortality rates from COVID-19 are high but appear to be decreasing for selected locations in the United States. It is not known whether this is because of changes in the characteristics of patients being admitted.
Objective: To describe changing in-hospital mortality rates over time after accounting for individual patient characteristics.
Design, setting, and participants: This was a retrospective cohort study of 20 736 adults with a diagnosis of COVID-19 who were included in the US American Heart Association COVID-19 Cardiovascular Disease Registry and admitted to 107 acute care hospitals in 31 states from March through November 2020. A multiple mixed-effects logistic regression was then used to estimate the odds of in-hospital death adjusted for patient age, sex, body mass index, and medical history as well as vital signs, use of supplemental oxygen, presence of pulmonary infiltrates at admission, and hospital site.
Main outcomes and measures: In-hospital death adjusted for exposures for 4 periods in 2020.
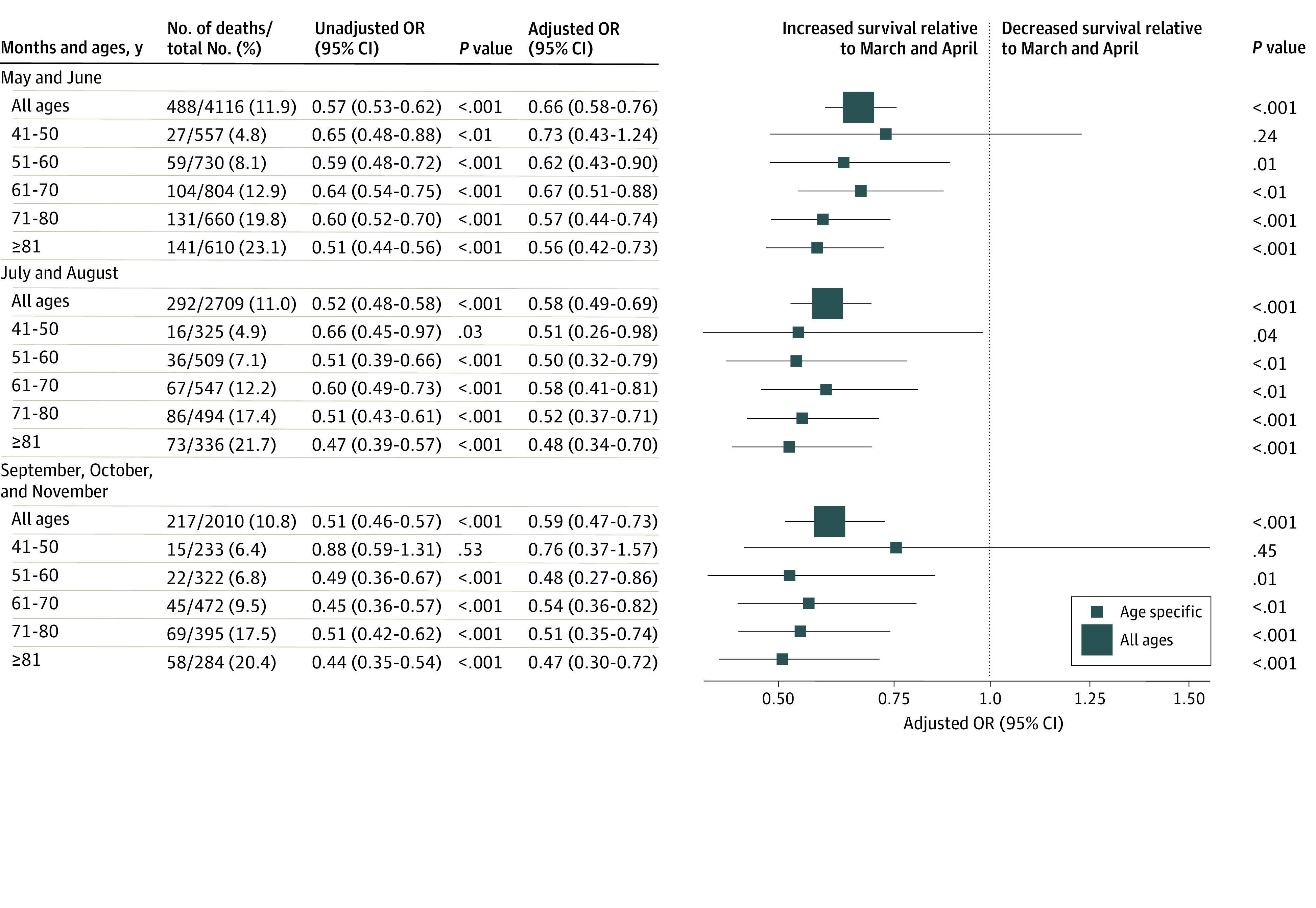
Results: The registry included 20 736 patients hospitalized with COVID-19 from March through November 2020 (9524 women [45.9%]; mean [SD] age, 61.2 [17.9] years); 3271 patients (15.8%) died in the hospital. Mortality rates were 19.1% in March and April, 11.9% in May and June, 11.0% in July and August, and 10.8% in September through November. Compared with March and April, the adjusted odds ratios for in-hospital death were significantly lower in May and June (odds ratio, 0.66; 95% CI, 0.58-0.76; P < .001), July and August (odds ratio, 0.58; 95% CI, 0.49-0.69; P < .001), and September through November (odds ratio, 0.59; 95% CI, 0.47-0.73).
Conclusions and relevance: In this cohort study, high rates of in-hospital COVID-19 mortality among registry patients in March and April 2020 decreased by more than one-third by June and remained near that rate through November. This difference in mortality rates between the months of March and April and later months persisted even after adjusting for age, sex, medical history, and COVID-19 disease severity and did not appear to be associated with changes in the characteristics of patients being admitted.
Conflict of interest statement
Figures
References
-
- Rodriguez F, Solomon N, de Lemos JA, et al. . Racial and ethnic differences in presentation and outcomes for patients hospitalized with COVID-19: findings from the American Heart Association's COVID-19 Cardiovascular Disease Registry. Published online November 17, 2020. Circulation. doi:10.1161/CIRCULATIONAHA.120.052278 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
