

Clinical and CT characteristics of Xpert MTB/RIF-negative pulmonary tuberculosis
- PMID: 33939723
- PMCID: PMC8092799
- DOI: 10.1371/journal.pone.0250616
Clinical and CT characteristics of Xpert MTB/RIF-negative pulmonary tuberculosis
Abstract
Purpose: To determine the diagnostic accuracy of the Xpert MTB/RIF assay in patients with smear-negative pulmonary tuberculosis (TB) and to assess clinical and CT characteristics of Xpert-negative pulmonary TB.
Material and methods: We retrospectively reviewed the records of 1,400 patients with suspected pulmonary TB for whom the sputum Xpert MTB/RIF assay was performed between September 1, 2014 and February 28, 2020. Clinical and CT characteristics of smear-negative pulmonary TB patients with negative Xpert MTB/RIF results were compared with positive results.
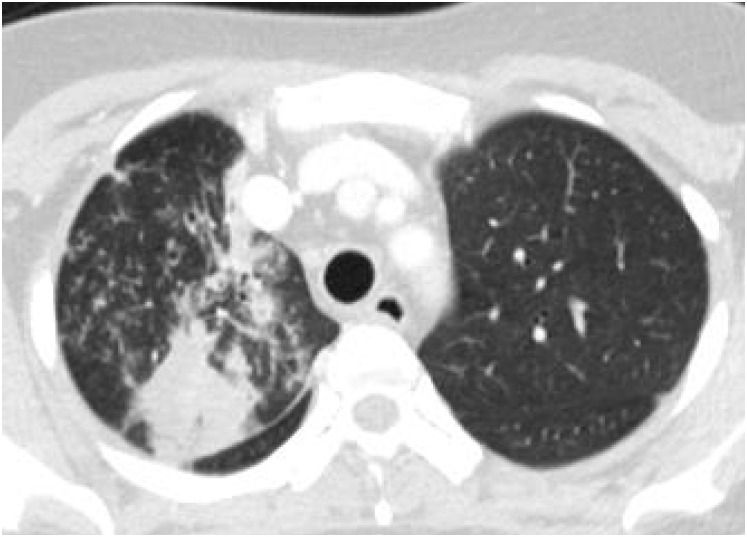
Results: Of 1,400 patients, 365 (26.1%) were diagnosed with pulmonary TB and 190 of 365 patients (52.1%) were negative for sputum acid-fast bacilli. The diagnosis of pulmonary TB was based on a positive culture, positive Xpert MTB/RIF or the clinical diagnoses of patients treated with an anti-TB medication. The sensitivity, specificity, positive predictive and negative predictive values of sputum Xpert MTB/RIF for smear-negative pulmonary TB were 41.1%, 100%, 100%, and 90.1%, respectively. Finally, 172 patients with smear-negative pulmonary TB who underwent chest CT within 2 weeks of diagnosis were included to compare Xpert-positive (n = 66) and Xpert- negative (n = 106) groups. Patients with sputum Xpert-negative TB showed lower positive rates for sputum culture (33.0% vs. 81.8%, p<0.001) and bronchoalveolar lavage culture (53.3% vs. 84.6%, p = 0.042) than in Xpert-positive TB. Time to start TB medication was longer in patients with Xpert-negative TB than in Xpert-positive TB (11.3±16.4 days vs. 5.0±8.7 days, p = 0.001). On chest CT, sputum Xpert-negative TB showed significantly lower frequency of consolidation (21.7% vs. 39.4%, p = 0.012), cavitation (23.6% vs. 37.9%, p = 0.045), more frequent peripheral location (50.9% vs. 21.2 p = 0.001) with lower area of involvement (4.3±4.3 vs. 7.6±6.4, p<0.001). Multivariate analysis revealed peripheral location (odds ratios, 2.565; 95% confidence interval: 1.157-5.687; p = 0.020) and higher total extent of the involved lobe (odds ratios, 0.928; 95% confidence interval: 0.865-0.995; p = 0.037) were significant factors associated with Xpert MTB/RIF-negative TB. Regardless of Xpert positivity, more than 80% of all cases were diagnosed of TB on chest CT by radiologists.
Conclusion: The detection rate of sputum Xpert MTB/RIF assay was relatively low for smear negative pulmonary TB. Chest CT image interpretation may play an important role in early diagnosis and treatment of Xpert MTB/RIF-negative pulmonary TB.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


Similar articles
-
Chest X-ray interpretation does not complement Xpert MTB/RIF in diagnosis of smear-negative pulmonary tuberculosis among TB-HIV co-infected adults in a resource-limited setting.BMC Infect Dis. 2021 Jan 13;21(1):63. doi: 10.1186/s12879-020-05752-7. BMC Infect Dis. 2021. PMID: 33435896 Free PMC article.
-
Xpert MTB/RIF assay in the diagnosis of pulmonary tuberculosis in children in tertiary care setting in South India.J Trop Pediatr. 2024 Aug 10;70(5):fmae024. doi: 10.1093/tropej/fmae024. J Trop Pediatr. 2024. PMID: 39152039
-
Evaluation of Xpert MTB/RIF Ultra performance for pulmonary tuberculosis diagnosis on smear-negative respiratory samples in a French centre.Eur J Clin Microbiol Infect Dis. 2019 Mar;38(3):601-605. doi: 10.1007/s10096-018-03463-1. Epub 2019 Jan 24. Eur J Clin Microbiol Infect Dis. 2019. PMID: 30680567
-
Systematic review: Comparison of Xpert MTB/RIF, LAMP and SAT methods for the diagnosis of pulmonary tuberculosis.Tuberculosis (Edinb). 2016 Jan;96:75-86. doi: 10.1016/j.tube.2015.11.005. Epub 2015 Nov 30. Tuberculosis (Edinb). 2016. PMID: 26786658
-
Stool Xpert MTB/RIF as a possible diagnostic alternative to sputum in Africa: a systematic review and meta-analysis.Front Public Health. 2023 May 24;11:1117709. doi: 10.3389/fpubh.2023.1117709. eCollection 2023. Front Public Health. 2023. PMID: 37293615 Free PMC article.
Cited by
-
Correlation Between CT Features of Active Tuberculosis and Residual Metabolic Activity on End-of-Treatment FDG PET/CT in Patients Treated for Pulmonary Tuberculosis.Front Med (Lausanne). 2022 Feb 22;9:791653. doi: 10.3389/fmed.2022.791653. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35295606 Free PMC article.
-
High prevalence and risk factors of positive sputum smear in newly diagnosed pulmonary tuberculosis patients in Vietnam.Infez Med. 2025 Jun 1;33(2):212-220. doi: 10.53854/liim-3302-7. eCollection 2025. Infez Med. 2025. PMID: 40519350 Free PMC article.
References
-
- Global Tuberculosis Report. World Health Organization.2018. https://apps.who.int/iris/handle/10665/274453.
-
- Diagnostic Standards and Classification of Tuberculosis in Adults and Children. This official statement of the American Thoracic Society and the Centers for Disease Control and Prevention was adopted by the ATS Board of Directors, July 1999. This statement was endorsed by the Council of the Infectious Disease Society of America, September 1999. Am J Respir Crit Care Med. 2000;161(4 Pt 1):1376–1395. 10.1164/ajrccm.161.4.16141 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
