

Ethnic differences in SARS-CoV-2 infection and COVID-19-related hospitalisation, intensive care unit admission, and death in 17 million adults in England: an observational cohort study using the OpenSAFELY platform
- PMID: 33939953
- PMCID: PMC8087292
- DOI: 10.1016/S0140-6736(21)00634-6
Ethnic differences in SARS-CoV-2 infection and COVID-19-related hospitalisation, intensive care unit admission, and death in 17 million adults in England: an observational cohort study using the OpenSAFELY platform
Erratum in
-
Department of Error.Lancet. 2021 Jun 12;397(10291):2252. doi: 10.1016/S0140-6736(21)01066-7. Epub 2021 May 6. Lancet. 2021. PMID: 33965069 Free PMC article. No abstract available.
Abstract
Background: COVID-19 has disproportionately affected minority ethnic populations in the UK. Our aim was to quantify ethnic differences in SARS-CoV-2 infection and COVID-19 outcomes during the first and second waves of the COVID-19 pandemic in England.
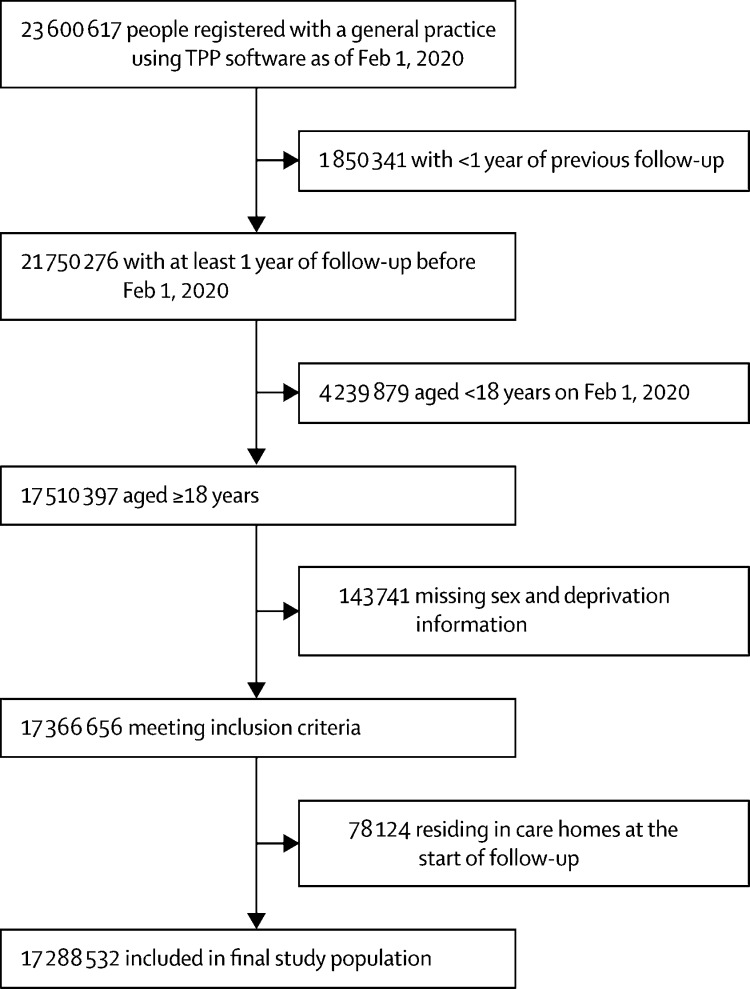
Methods: We conducted an observational cohort study of adults (aged ≥18 years) registered with primary care practices in England for whom electronic health records were available through the OpenSAFELY platform, and who had at least 1 year of continuous registration at the start of each study period (Feb 1 to Aug 3, 2020 [wave 1], and Sept 1 to Dec 31, 2020 [wave 2]). Individual-level primary care data were linked to data from other sources on the outcomes of interest: SARS-CoV-2 testing and positive test results and COVID-19-related hospital admissions, intensive care unit (ICU) admissions, and death. The exposure was self-reported ethnicity as captured on the primary care record, grouped into five high-level census categories (White, South Asian, Black, other, and mixed) and 16 subcategories across these five categories, as well as an unknown ethnicity category. We used multivariable Cox regression to examine ethnic differences in the outcomes of interest. Models were adjusted for age, sex, deprivation, clinical factors and comorbidities, and household size, with stratification by geographical region.
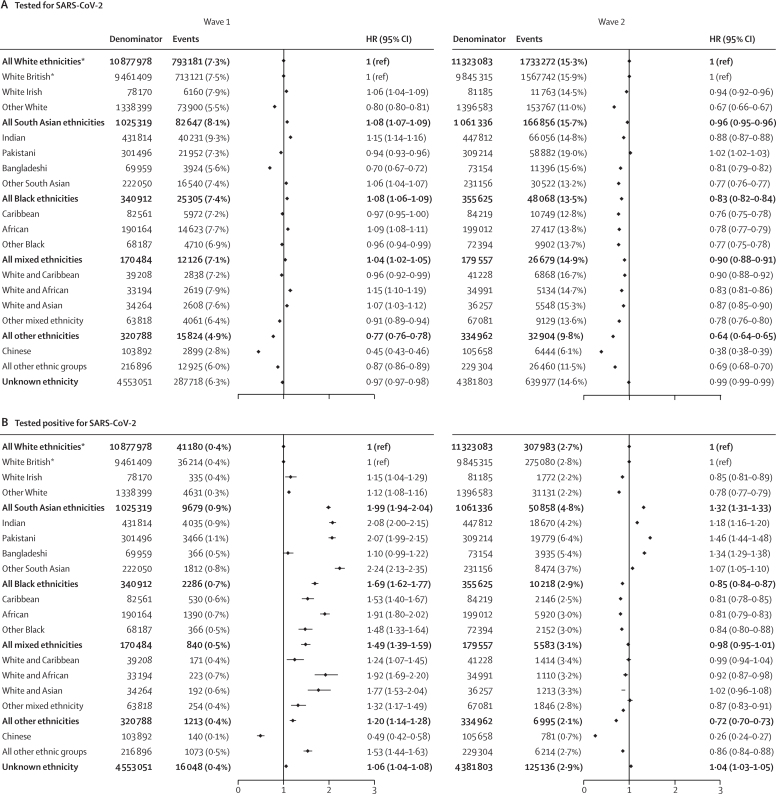
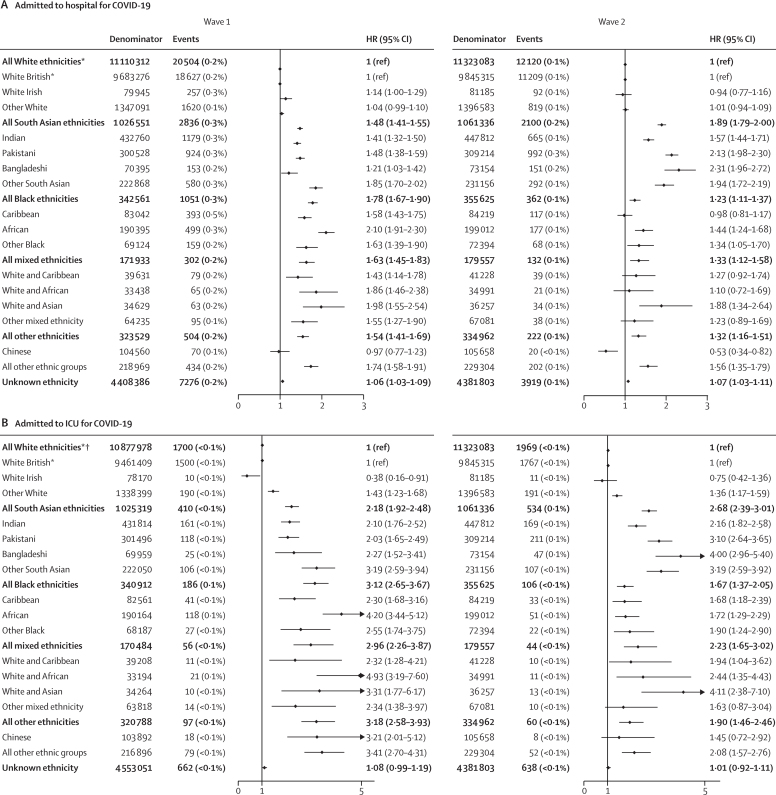
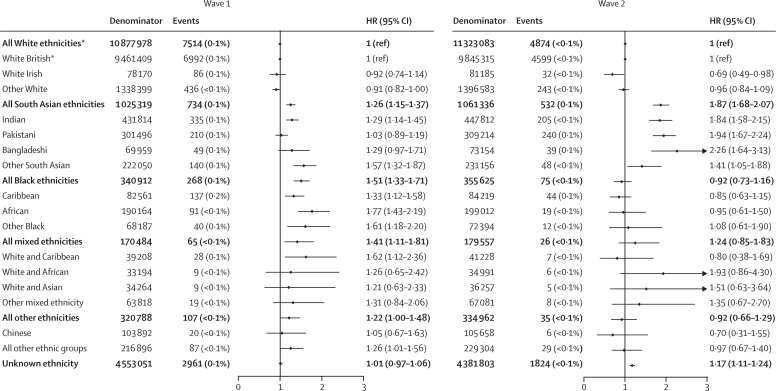
Findings: Of 17 288 532 adults included in the study (excluding care home residents), 10 877 978 (62·9%) were White, 1 025 319 (5·9%) were South Asian, 340 912 (2·0%) were Black, 170 484 (1·0%) were of mixed ethnicity, 320 788 (1·9%) were of other ethnicity, and 4 553 051 (26·3%) were of unknown ethnicity. In wave 1, the likelihood of being tested for SARS-CoV-2 infection was slightly higher in the South Asian group (adjusted hazard ratio 1·08 [95% CI 1·07-1·09]), Black group (1·08 [1·06-1·09]), and mixed ethnicity group (1·04 [1·02-1·05]) and was decreased in the other ethnicity group (0·77 [0·76-0·78]) relative to the White group. The risk of testing positive for SARS-CoV-2 infection was higher in the South Asian group (1·99 [1·94-2·04]), Black group (1·69 [1·62-1·77]), mixed ethnicity group (1·49 [1·39-1·59]), and other ethnicity group (1·20 [1·14-1·28]). Compared with the White group, the four remaining high-level ethnic groups had an increased risk of COVID-19-related hospitalisation (South Asian group 1·48 [1·41-1·55], Black group 1·78 [1·67-1·90], mixed ethnicity group 1·63 [1·45-1·83], other ethnicity group 1·54 [1·41-1·69]), COVID-19-related ICU admission (2·18 [1·92-2·48], 3·12 [2·65-3·67], 2·96 [2·26-3·87], 3·18 [2·58-3·93]), and death (1·26 [1·15-1·37], 1·51 [1·31-1·71], 1·41 [1·11-1·81], 1·22 [1·00-1·48]). In wave 2, the risks of hospitalisation, ICU admission, and death relative to the White group were increased in the South Asian group but attenuated for the Black group compared with these risks in wave 1. Disaggregation into 16 ethnicity groups showed important heterogeneity within the five broader categories.
Interpretation: Some minority ethnic populations in England have excess risks of testing positive for SARS-CoV-2 and of adverse COVID-19 outcomes compared with the White population, even after accounting for differences in sociodemographic, clinical, and household characteristics. Causes are likely to be multifactorial, and delineating the exact mechanisms is crucial. Tackling ethnic inequalities will require action across many fronts, including reducing structural inequalities, addressing barriers to equitable care, and improving uptake of testing and vaccination.
Funding: Medical Research Council.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests BG has received research funding from Health Data Research UK, the Laura and John Arnold Foundation, the Wellcome Trust, the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre, the NHS NIHR School of Primary Care Research, the Mohn-Westlake Foundation, the Good Thinking Foundation, the Health Foundation, and WHO; and receives personal income from speaking and writing for lay audiences on the misuse of science. IJD has received unrestricted research grants from and holds shares in GlaxoSmithKline. KK is the director for the University of Leicester Centre for BME Health, Trustee of the South Asian Health Foundation, the NIHR Applied Research Collaboration lead for Ethnicity and Diversity, and a member of the Independent Scientific Advisory Group for Emergencies (SAGE) and chair for the SAGE Ethnicity Subgroup. RM, BG, and RME are members of the SAGE Ethnicity Subgroup. RM reports personal fees from AMGEN. AS is employed by the London School of Hygiene & Tropical Medicine (LSHTM) on a fellowship sponsored by GlaxoSmithKline. All other authors declare no competing interests.
Figures
Comment in
-
COVID-19 and disparities affecting ethnic minorities.Lancet. 2021 May 8;397(10286):1684-1685. doi: 10.1016/S0140-6736(21)00949-1. Epub 2021 Apr 30. Lancet. 2021. PMID: 33939952 Free PMC article. No abstract available.
-
COVID-19: counting migrants in.Lancet. 2021 Jul 17;398(10296):211-212. doi: 10.1016/S0140-6736(21)01339-8. Lancet. 2021. PMID: 34274061 Free PMC article. No abstract available.
-
Ethnic disparities in COVID-19: increased risk of infection or severe disease? - Authors' reply.Lancet. 2021 Jul 31;398(10298):390. doi: 10.1016/S0140-6736(21)01424-0. Lancet. 2021. PMID: 34332682 Free PMC article. No abstract available.
References
-
- Public Health England Beyond the data: understanding the impact of COVID-19 on BAME groups. June, 2020. https://assets.publishing.service.gov.uk/government/uploads/system/uploa...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
