

Galcanezumab for the prevention of high frequency episodic and chronic migraine in real life in Italy: a multicenter prospective cohort study (the GARLIT study)
- PMID: 33941080
- PMCID: PMC8091153
- DOI: 10.1186/s10194-021-01247-1
Galcanezumab for the prevention of high frequency episodic and chronic migraine in real life in Italy: a multicenter prospective cohort study (the GARLIT study)
Abstract
Background: The clinical benefit of galcanezumab, demonstrated in randomized clinical trials (RCTs), remains to be quantified in real life. This study aimed at evaluating the effectiveness, safety and tolerability of galcanezumab in the prevention of high-frequency episodic migraine (HFEM) and chronic migraine (CM) in a real-life setting.
Methods: This multicenter prospective observational cohort study was conducted between November 2019 and January 2021 at 13 Italian headache centers. Consecutive adult HFEM and CM patients clinically eligible were enrolled and treated with galcanezumab subcutaneous injection 120 mg monthly with the first loading dose of 240 mg. The primary endpoint was the change in monthly migraine days (MMDs) in HFEM and monthly headache days (MHDs) in CM patients after 6 months of therapy (V6). Secondary endpoints were the Numerical Rating Scale (NRS), monthly painkiller intake (MPI), HIT-6 and MIDAS scores changes, ≥50% responder rates (RR), the conversion rate from CM to episodic migraine (EM) and Medication Overuse (MO) discontinuation.
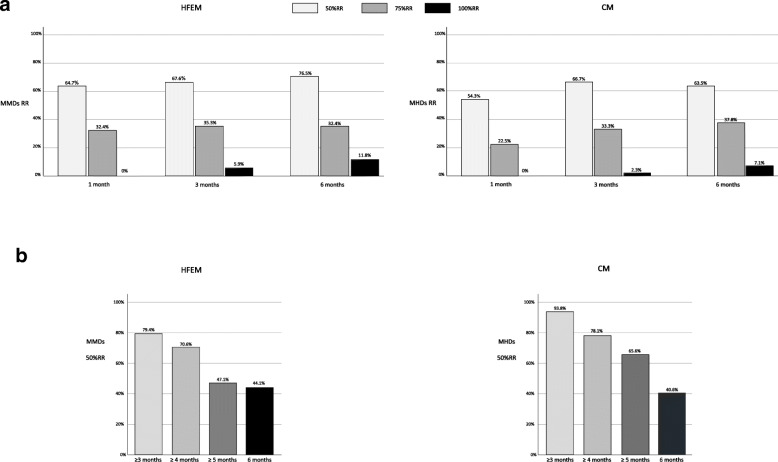
Results: One hundred sixty-three patients (80.5% female, 47.1 ± 11.7 years, 79.8% CM) were included. At V6, MMDs reduced by 8 days in HFEM and MHDs by 13 days in CM patients (both p < .001). NRS, MPI, HIT-6 and MIDAS scores significantly decreased (p < .001). Ten patients (6.1%) dropped out for inefficacy and classified as non-responders. Patients with ≥50%RRs, i.e. responders, were 76.5% in the HFEM and 63.5% in the CM group at V6. Among CM patients, the V6 responders presented a lower body mass index (p = .018) and had failed a lower number of preventive treatments (p = .013) than non-responders. At V6, 77.2% of CM patients converted to EM, and 82.0% ceased MO. Adverse events, none serious, were reported in up to 10.3% of patients during evaluation times.
Conclusions: Galcanezumab in real life was safe, well tolerated and seemed more effective than in RCTs. Normal weight and a low number of failed preventives were positively associated with galcanezumab effectiveness in CM patients.
Trial registration: ClinicalTrials.gov NCT04803513 .
Keywords: Calcitonin gene-related peptide; Migraine treatment; Monoclonal antibodies; Real world.
Conflict of interest statement
Fabrizio Vernieri received travel grants, honoraria for advisory boards, speaker panels, or clinical investigation studies from Allergan, Amgen, Angelini, Eli-Lilly, Lundbeck, Novartis, and Teva. Claudia Altamura received grants and honoraria from Novartis, Eli Lilly. Cinzia Aurilia received travel grants and honoraria from FB-Health, Lusofarmaco, Almirall, Eli-Lilly Novartis and Teva. Gabriella Egeo received travel grants and honoraria from Eli-Lilly, Novartis, New Penta and Ecupharma. Luisa Fofi received travel grants and honoraria from Teva, Eli-Lilly and Novartis. Valentina Favoni received honoraria as speaker or for participating in advisory boards from Ely-Lilly, Novartis and Teva. Giulia Pierangeli received grants and honoraria from Teva, Lilly, Allergan, Novartis, Lundbeck, Amgen, IBSA. Carlo Lovati received grants from Novartis and Lilly. Marco Aguggia received grants from Novartis and Lilly. Florindo d’Onofrio received grants and honoraria from Lilly, Teva, Novartis, Neopharmed. Alberto Doretti received grants and honoraria from Novartis, Eli Lilly. Paola Di Fiore received grants and honoraria from Teva, Novartis, IBSA. Cinzia Finocchi received grants and honoraria from Novartis, Eli Lilly, AIM group. Renata Rao received honoraria for speaker panels from Teva, Lilly, Novartis. Francesco Bono received honoraria as a speaker or for participating in advisory boards from Teva, Novartis, Ipsen. Angelo Ranieri received speaker honoraria from Teva, Lilly. Sabina Cevoli received travel grants, honoraria for advisory boards, speaker panels or clinical investigation studies from Novartis, Teva, Lilly, Allergan, Ibsa, Amgen and Lundbeck. Piero Barbanti received travel grants, honoraria for advisory boards, speaker panels or clinical investigation studies from Alder, Allergan, Angelini, Bayer, ElectroCore, Eli-Lilly, GSK, Lusofarmaco, MSD, Novartis, Stx-Med, Teva, Visufarma, Zambon. Nicoletta Brunelli, Carmelina Maria Costa, Maria Albanese have nothing to disclose.
Figures



References
-
- Stovner LJ, Nichols E, Steiner TJ, Abd-Allah F, Abdelalim A, al-Raddadi RM, Ansha MG, Barac A, Bensenor IM, Doan LP, Edessa D, Endres M, Foreman KJ, Gankpe FG, Gopalkrishna G, Goulart AC, Gupta R, Hankey GJ, Hay SI, Hegazy MI, Hilawe EH, Kasaeian A, Kassa DH, Khalil I, Khang YH, Khubchandan J, Kim YJ, Kokubo Y, Mohammed MA, Moradi-Lakeh M, Nguyen HLT, Nirayo YL, Qorbani M, Ranta A, Roba KT, Safiri S, Santos IS, Satpathy M, Sawhney M, Shiferaw MS, Shiue I, Smith M, Szoeke CEI, Truong NT, Venketasubramanian N, Weldegwergs K, Westerman R, Wijeratne T, Tran BX, Yonemoto N, Feigin VL, Vos T, Murray CJL. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. 2018;17(11):954–976. - PMC - PubMed
-
- Lipton RB, Bigal ME, Diamond M, Freitag F, Reed ML, Stewart WF, on behalf of the AMPP Advisory Group Migraine prevalence, disease burden, and the need for preventive therapy. Neurology. 2007;68(5):343–349. - PubMed
-
- Silberstein SD, Holland S, Freitag F, Dodick DW, Argoff C, Ashman E, Quality Standards Subcommittee of the American Academy of Neurology and the American Headache Society Evidence-based guideline update: pharmacologic treatment for episodic migraine prevention in adults: table 1. Neurology. 2012;78(17):1337–1345. - PMC - PubMed
-
- Evers S, Áfra J, Frese A, et al. EFNS guideline on the drug treatment of migraine - revised report of an EFNS task force. Eur J Neurol. 2009;16(9):968–981. - PubMed
-
- Silberstein SD, Lipton RB, Dodick DW, Freitag FG, Ramadan N, Mathew N, Brandes JL, Bigal M, Saper J, Ascher S, Jordan DM, Greenberg SJ, Hulihan J, on behalf of the Topiramate Chronic Migraine Study Group Efficacy and safety of topiramate for the treatment of chronic migraine: a randomized, double-blind, placebo-controlled trial. Headache. 2007;47(2):170–180. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
