

Impact of HER2 Heterogeneity on Treatment Response of Early-Stage HER2-Positive Breast Cancer: Phase II Neoadjuvant Clinical Trial of T-DM1 Combined with Pertuzumab
- PMID: 33941592
- PMCID: PMC8598376
- DOI: 10.1158/2159-8290.CD-20-1557
Impact of HER2 Heterogeneity on Treatment Response of Early-Stage HER2-Positive Breast Cancer: Phase II Neoadjuvant Clinical Trial of T-DM1 Combined with Pertuzumab
Abstract
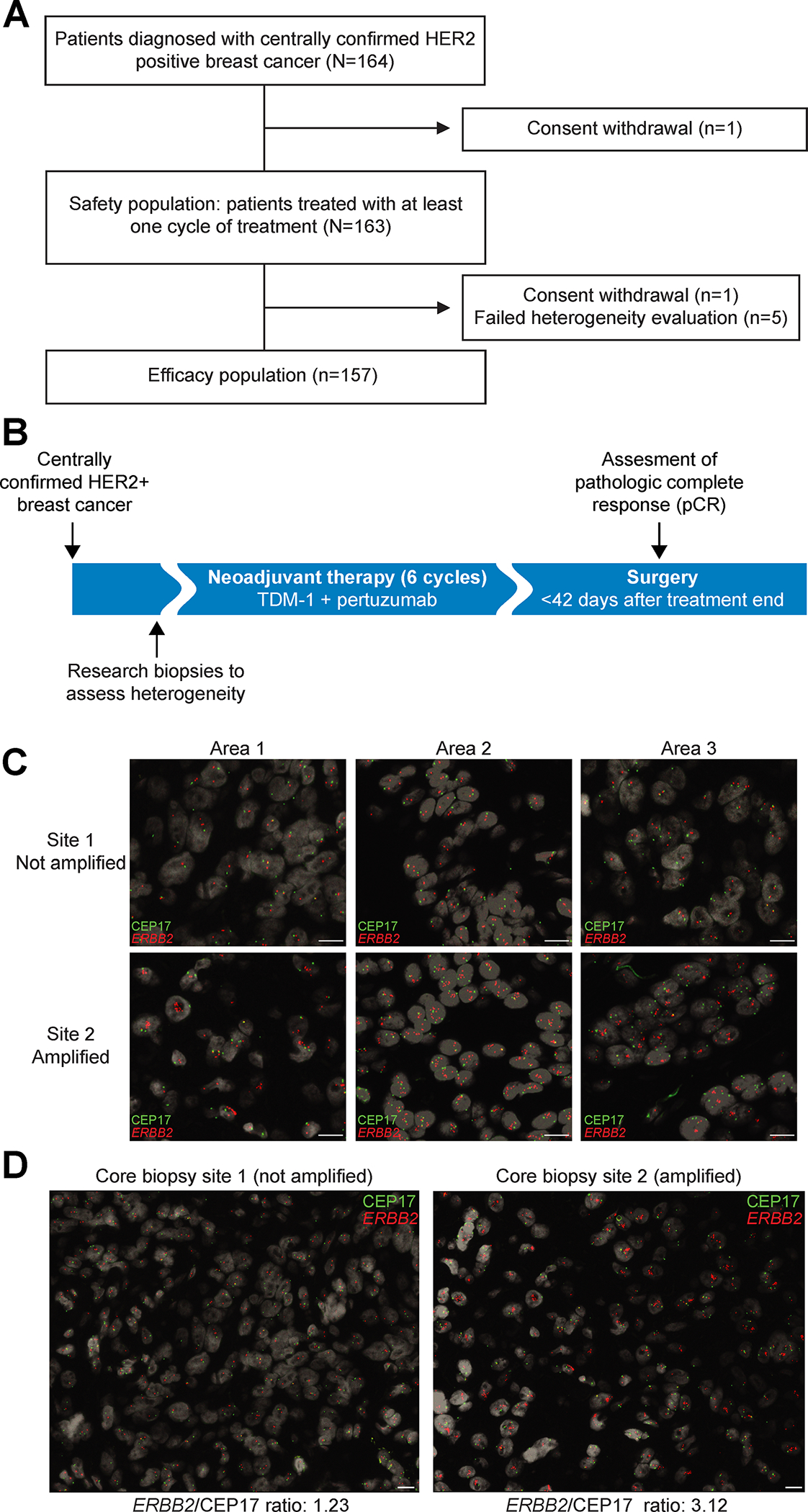
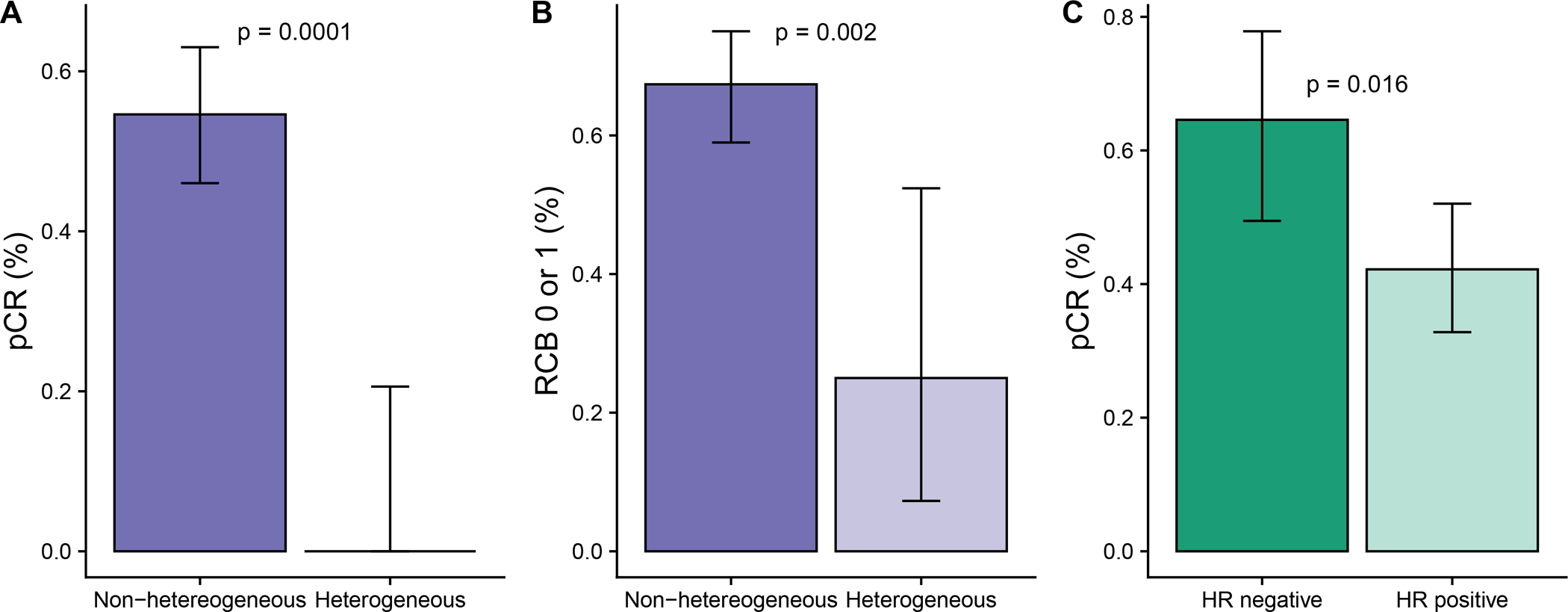
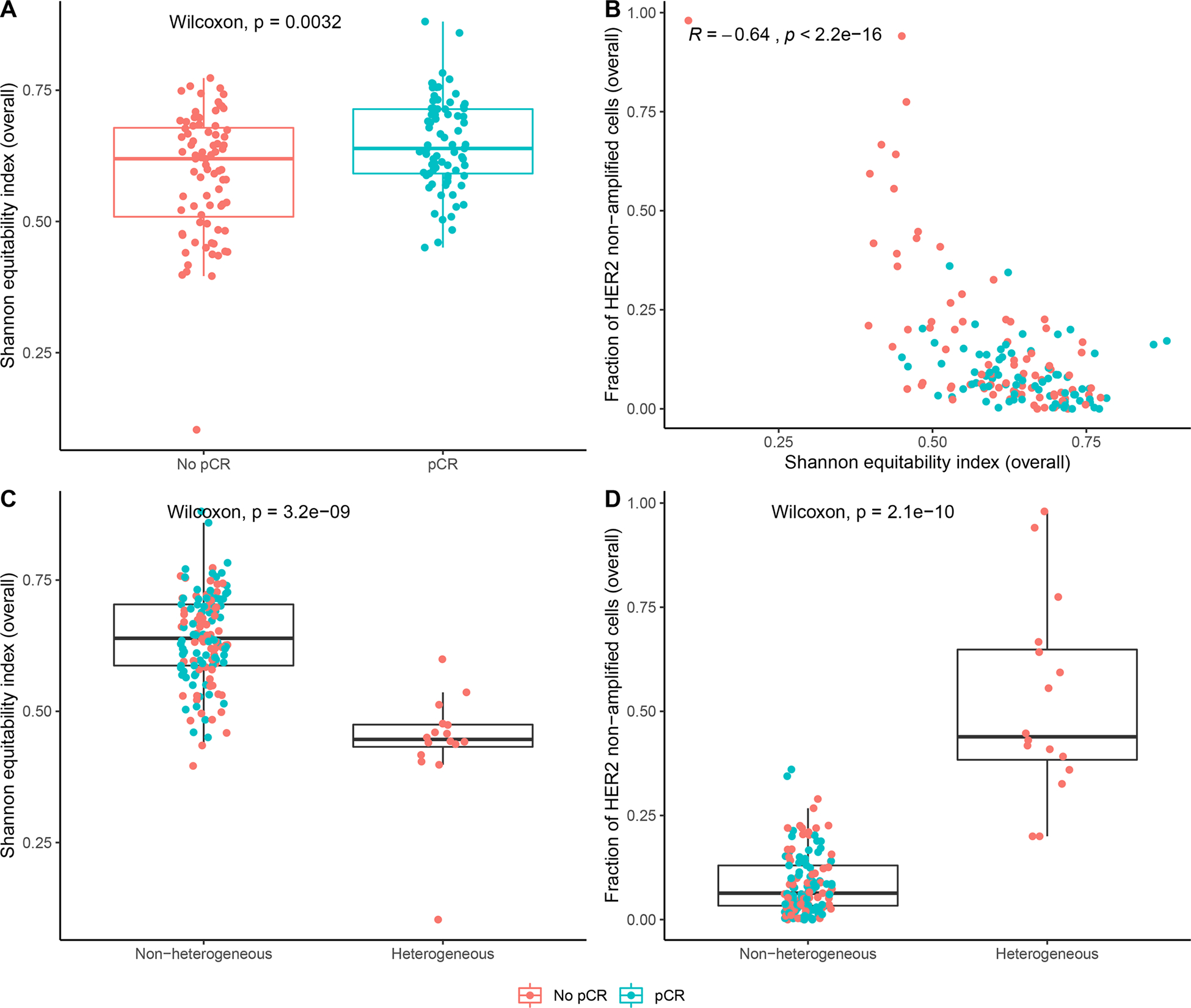
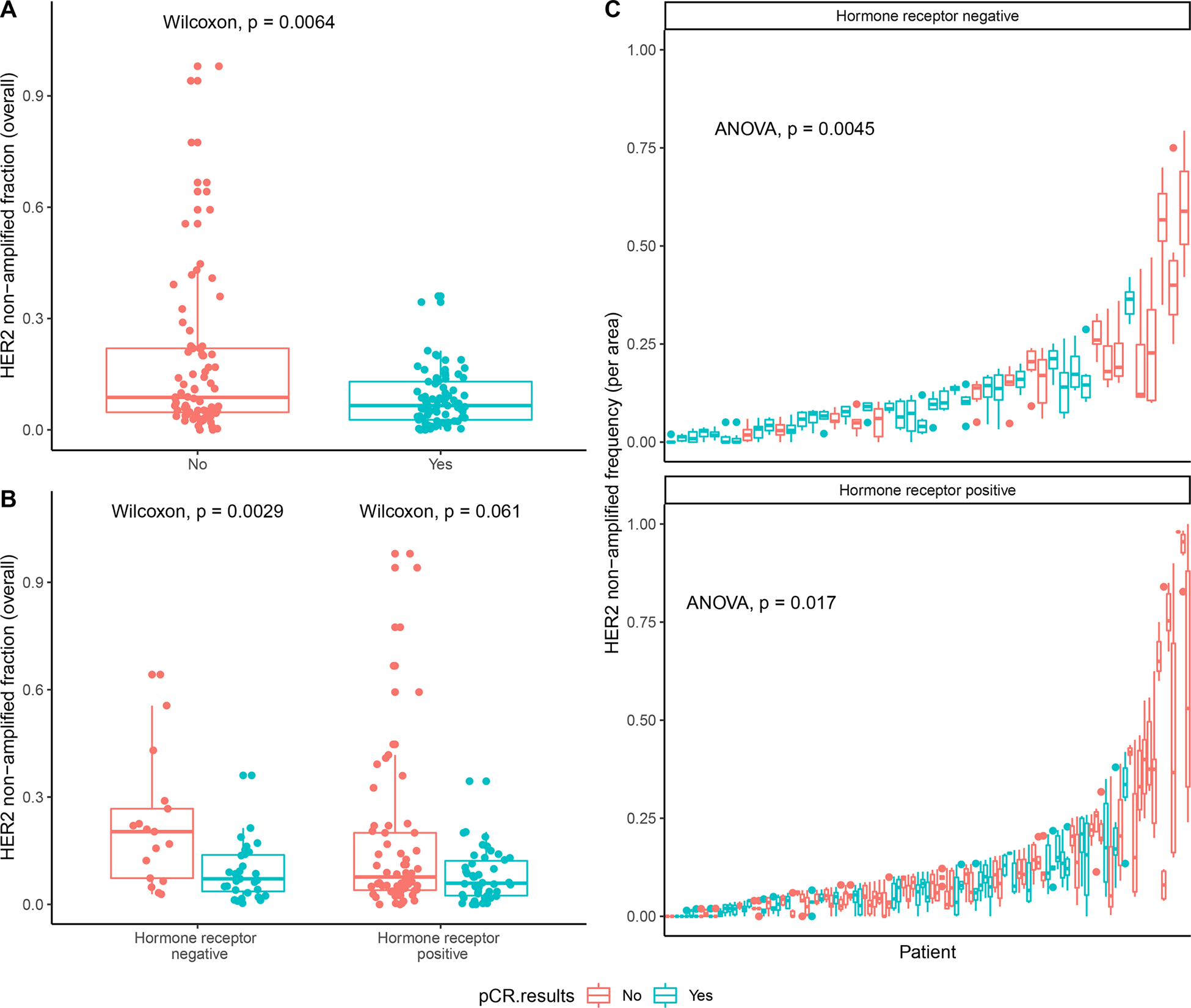
Intratumor heterogeneity is postulated to cause therapeutic resistance. To prospectively assess the impact of HER2 (ERBB2) heterogeneity on response to HER2-targeted therapy, we treated 164 patients with centrally confirmed HER2-positive early-stage breast cancer with neoadjuvant trastuzumab emtansine plus pertuzumab. HER2 heterogeneity was assessed on pretreatment biopsies from two locations of each tumor. HER2 heterogeneity, defined as an area with ERBB2 amplification in >5% but <50% of tumor cells, or a HER2-negative area by FISH, was detected in 10% (16/157) of evaluable cases. The pathologic complete response rate was 55% in the nonheterogeneous subgroup and 0% in the heterogeneous group (P < 0.0001, adjusted for hormone receptor status). Single-cell ERBB2 FISH analysis of cellular heterogeneity identified the fraction of ERBB2 nonamplified cells as a driver of therapeutic resistance. These data suggest HER2 heterogeneity is associated with resistance to HER2-targeted therapy and should be considered in efforts to optimize treatment strategies. SIGNIFICANCE: HER2-targeted therapies improve cure rates in HER2-positive breast cancer, suggesting chemotherapy can be avoided in a subset of patients. We show that HER2 heterogeneity, particularly the fraction of ERBB2 nonamplified cancer cells, is a strong predictor of resistance to HER2 therapies and could potentially be used to optimize treatment selection.See related commentary by Okines and Turner, p. 2369.This article is highlighted in the In This Issue feature, p. 2355.
©2021 American Association for Cancer Research.
Figures
Comment in
-
Heterogeneous HER2 Amplification-a New Clinical Category of HER2-Positive Breast Cancer?Cancer Discov. 2021 Oct;11(10):2369-2371. doi: 10.1158/2159-8290.CD-21-0936. Cancer Discov. 2021. PMID: 34598949
References
-
- King CR, Kraus MH, Aaronson SA. Amplification of a novel v-erbB-related gene in a human mammary carcinoma. Science 1985;229(4717):974–6. - PubMed
-
- Slamon DJ, Clark GM, Wong SG, Levin WJ, Ullrich A, McGuire WL. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 1987;235(4785):177–82. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
