

Phase I Trial of Cemiplimab, Radiotherapy, Cyclophosphamide, and Granulocyte Macrophage Colony-Stimulating Factor in Patients with Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma
- PMID: 33942954
- PMCID: PMC8417861
- DOI: 10.1002/onco.13810
Phase I Trial of Cemiplimab, Radiotherapy, Cyclophosphamide, and Granulocyte Macrophage Colony-Stimulating Factor in Patients with Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma
Abstract
Lessons learned: Cemiplimab in combination with radiation therapy, cyclophosphamide, and granulocyte macrophage colony-stimulating factor did not demonstrate efficacy above what can be achieved with other PD-1 inhibitor monotherapies in patients with refractory and metastatic head and neck squamous cell carcinoma. The safety profile of cemiplimab combination therapy was consistent with previously reported safety profiles of cemiplimab monotherapy. No new safety signal was observed.
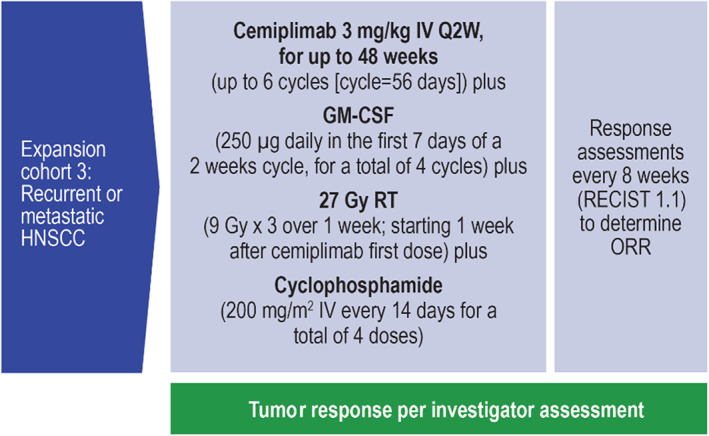
Background: Refractory and metastatic (R/M) head and neck squamous cell carcinoma (HNSCC) generally does not respond to PD-1 inhibitor monotherapy. Cemiplimab is a human anti-PD-1 monoclonal antibody. An expansion cohort enrolled patients with R/M HNSCC in a phase I study combining cemiplimab plus radiation therapy (RT), cyclophosphamide, and granulocyte macrophage colony-stimulating factor (GM-CSF).
Methods: Patients with R/M HNSCC refractory to at least first-line therapy and for whom palliative RT is clinically indicated received cemiplimab plus RT, cyclophosphamide, and GM-CSF. The co-primary objectives were the safety, tolerability, and efficacy of cemiplimab plus RT, cyclophosphamide, and GM-CSF in 15 patients with R/M HNSCC.
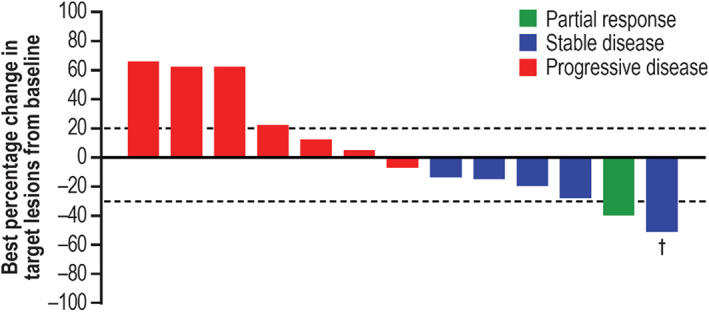
Results: Fifteen patients were enrolled. Patients discontinued treatment due to progression of disease. The most common treatment-emergent adverse events (TEAEs) of any grade were fatigue (40.0%), constipation (26.7%), and asthenia, dyspnea, maculo-papular rash, and pneumonia (each 20%). The only grade ≥3 TEAE that occurred in two patients was pneumonia (13.3%). By investigator assessment, there was one partial response (6.7%); disease control rate was 40.0% (95% confidence interval [CI], 16.3-67.7; five patients with stable disease); seven patients had progressive disease, and two were not evaluable. Median progression-free survival by investigator assessment was 1.8 months (95% CI, 1.7-4.7).
Conclusion: The regimen demonstrated tolerability but not efficacy above that which can be achieved with anti-PD-1 inhibitor monotherapy for R/M HNSCC.
Trial registration: ClinicalTrials.gov NCT02383212.
Keywords: Cemiplimab; Head and neck; Radiotherapy.
© AlphaMed Press; the data published online to support this summary are the property of the authors.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
