

The synergistic efficacy of hydroxychloroquine with methotrexate is accompanied by increased erythrocyte mean corpuscular volume
- PMID: 33944915
- PMCID: PMC8824424
- DOI: 10.1093/rheumatology/keab403
The synergistic efficacy of hydroxychloroquine with methotrexate is accompanied by increased erythrocyte mean corpuscular volume
Abstract
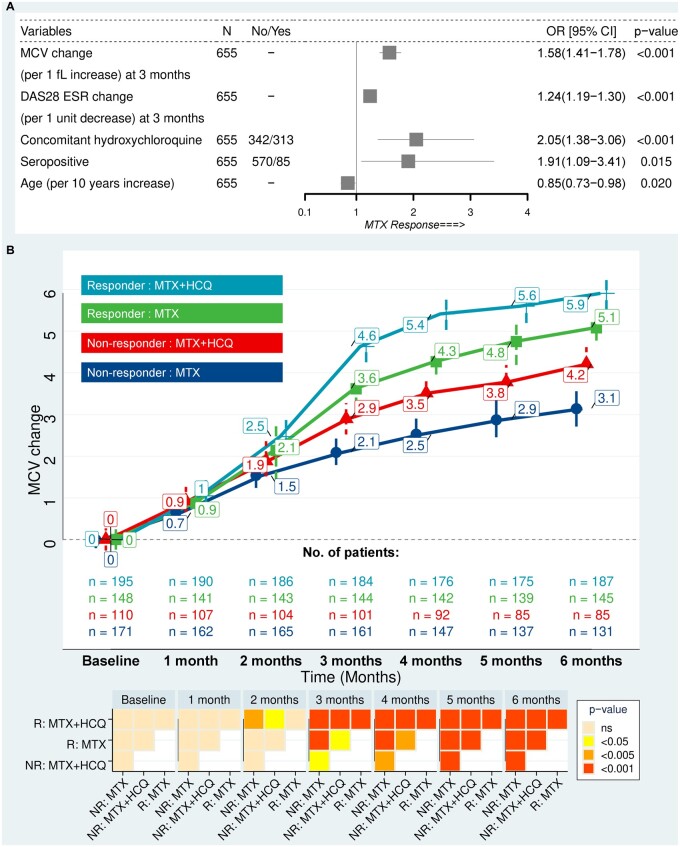
Objectives: To determine whether concomitant HCQ modulates the increase in erythrocyte mean corpuscular volume (MCV) caused by MTX therapy, and whether this is associated with improved clinical response in RA.
Methods: A retrospective observational analysis was conducted on two independent hospital datasets of biologic-naïve, early-RA patients who started oral MTX. Baseline characteristics, DAS28-ESR and monthly MCV after starting MTX were obtained. Conventional and machine-learning statistical approaches were applied to the discovery cohort (Cohort 1, 655 patients) and results validated using Cohort 2 (225 patients).
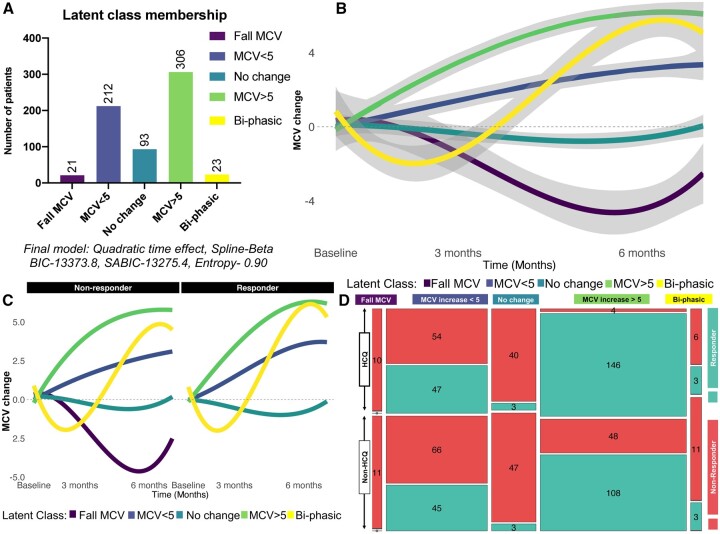
Results: HCQ therapy with MTX was associated with a 2-fold increase in the likelihood of response defined in this study as clinical remission or low disease activity at 6 months (P <0.001). The improved clinical outcome of combination HCQ and MTX therapy was associated with an accelerated rise in MCV from 2 months after commencing therapy. The increase in MCV at 3 months was equivalent to the contemporaneous reduction in the DAS (DAS28-ESR) in predicting clinical response at 6 months. Using latent class mixed modelling, five trajectories of MCV change over 6 months from baseline were identified. The odds ratio of response to treatment was 16.2 (95% CI 5.7, 46.4, P <0.001) in those receiving combination therapy classified within the MCV elevation >5 fl class, which contained the most patients, compared with MTX alone.
Conclusion: Our data provide mechanistic insight into the synergistic clinical benefit of concomitant HCQ with MTX, boosting the rise in MCV, which could serve as a companion biomarker of treatment response.
Keywords: HCQ; MTX; biomarker; mean corpuscular change; synergistic.
© The Author(s) 2021. Published by Oxford University Press on behalf of the British Society for Rheumatology.
Figures
References
-
- Smolen JS, Landewé RBM, Bijlsma JWJ et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis 2020;79:685–99. - PubMed
-
- Singh JA, Saag KG, Bridges SL Jr et al. 2015 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol 2016;68:1–26. - PubMed
-
- Verschueren P, De Cock D, Corluy L et al. Methotrexate in combination with other DMARDs is not superior to methotrexate alone for remission induction with moderate-to-high-dose glucocorticoid bridging in early rheumatoid arthritis after 16 weeks of treatment: the CareRA trial. Ann Rheum Dis 2015;74:27–34. - PubMed
-
- Hazlewood GS, Barnabe C, Tomlinson G et al. Methotrexate monotherapy and methotrexate combination therapy with traditional and biologic disease modifying antirheumatic drugs for rheumatoid arthritis: abridged Cochrane systematic review and network meta-analysis. BMJ (Clin Res Ed) 2016;353:i1777. - PMC - PubMed
-
- Schapink L, van den Ende CHM, Gevers LAHA, van Ede AE, den Broeder AA. The effects of methotrexate and hydroxychloroquine combination therapy vs methotrexate monotherapy in early rheumatoid arthritis patients. Rheumatology (Oxford) 2018;58:131–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
