

Relationship of SARS-CoV-2-specific CD4 response to COVID-19 severity and impact of HIV-1 and tuberculosis coinfection
- PMID: 33945513
- PMCID: PMC8203446
- DOI: 10.1172/JCI149125
Relationship of SARS-CoV-2-specific CD4 response to COVID-19 severity and impact of HIV-1 and tuberculosis coinfection
Abstract
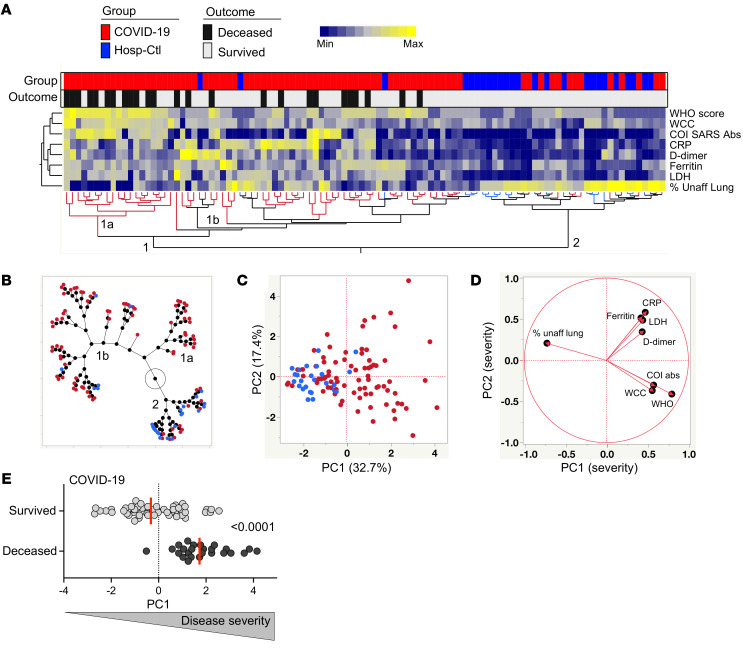
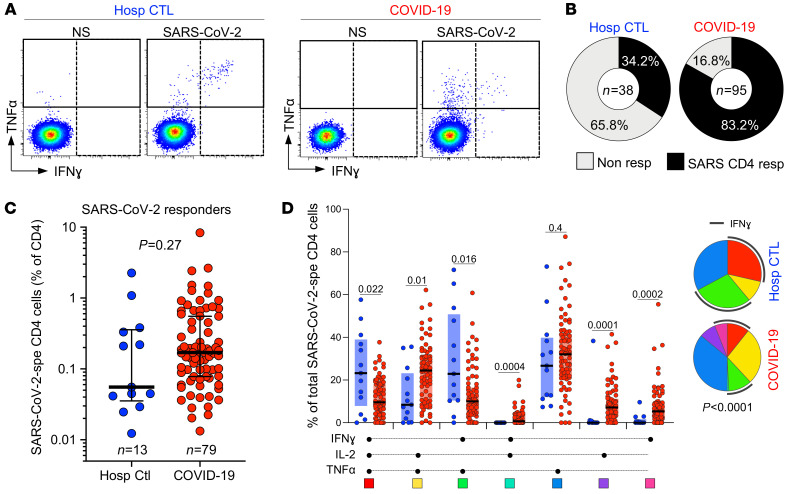
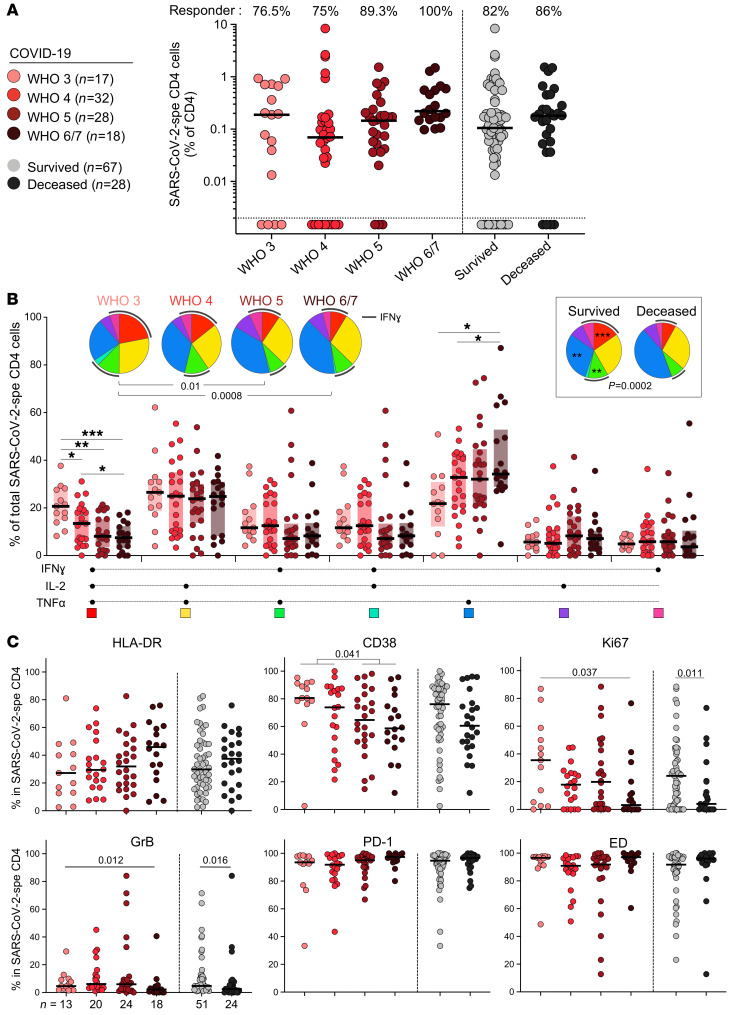
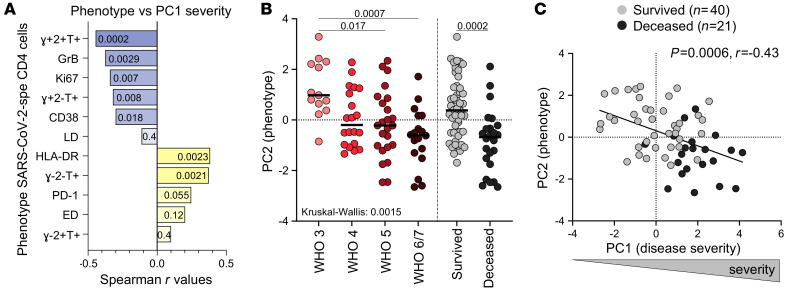
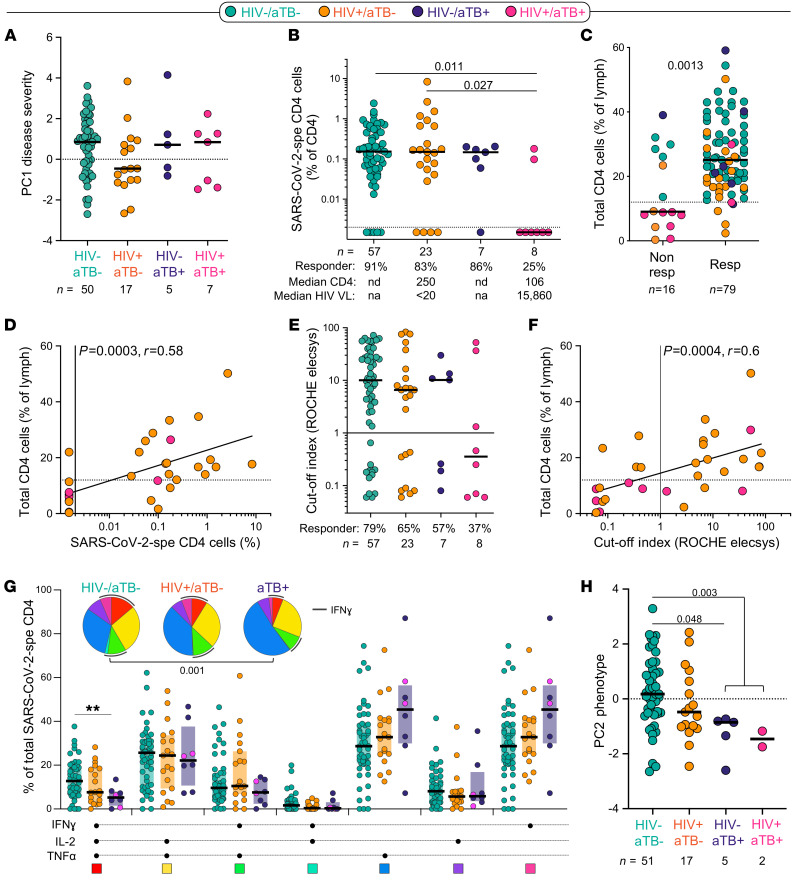
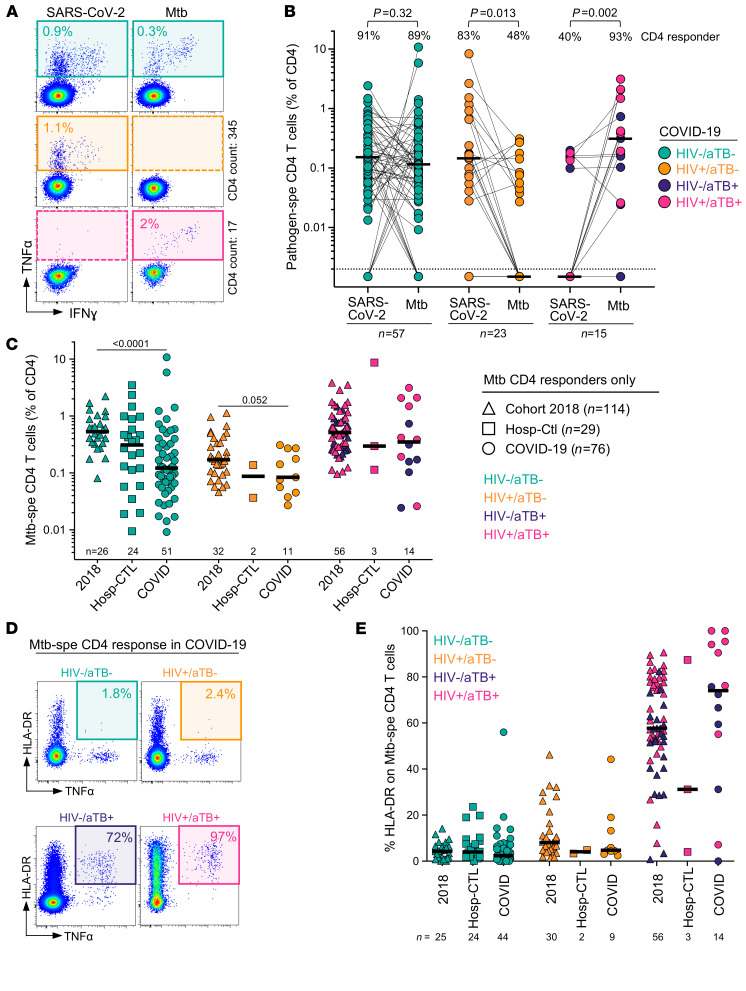
T cells are involved in control of coronavirus disease 2019 (COVID-19), but limited knowledge is available on the relationship between antigen-specific T cell response and disease severity. Here, we used flow cytometry to assess the magnitude, function, and phenotype of SARS coronavirus 2-specific (SARS-CoV-2-specific) CD4+ T cells in 95 hospitalized COVID-19 patients, 38 of them being HIV-1 and/or tuberculosis (TB) coinfected, and 38 non-COVID-19 patients. We showed that SARS-CoV-2-specific CD4+ T cell attributes, rather than magnitude, were associated with disease severity, with severe disease being characterized by poor polyfunctional potential, reduced proliferation capacity, and enhanced HLA-DR expression. Moreover, HIV-1 and TB coinfection skewed the SARS-CoV-2 T cell response. HIV-1-mediated CD4+ T cell depletion associated with suboptimal T cell and humoral immune responses to SARS-CoV-2, and a decrease in the polyfunctional capacity of SARS-CoV-2-specific CD4+ T cells was observed in COVID-19 patients with active TB. Our results also revealed that COVID-19 patients displayed reduced frequency of Mycobacterium tuberculosis-specific CD4+ T cells, with possible implications for TB disease progression. These results corroborate the important role of SARS-CoV-2-specific T cells in COVID-19 pathogenesis and support the concept of altered T cell functions in patients with severe disease.
Keywords: AIDS/HIV; COVID-19; Cellular immune response; T cells; Tuberculosis.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
