

α2-Adrenergic Agonists or Stimulants for Preschool-Age Children With Attention-Deficit/Hyperactivity Disorder
- PMID: 33946100
- PMCID: PMC8097628
- DOI: 10.1001/jama.2021.6118
α2-Adrenergic Agonists or Stimulants for Preschool-Age Children With Attention-Deficit/Hyperactivity Disorder
Erratum in
-
Error in Results.JAMA. 2021 Oct 12;326(14):1440. doi: 10.1001/jama.2021.16131. JAMA. 2021. PMID: 34636871 Free PMC article. No abstract available.
-
Corrected Classification of Drugs in Table.JAMA. 2024 Jul 16;332(3):257. doi: 10.1001/jama.2024.11398. JAMA. 2024. PMID: 38884984 Free PMC article. No abstract available.
Abstract
Importance: Attention-deficit/hyperactivity disorder (ADHD) is diagnosed in approximately 2.4% of preschool-age children. Stimulants are recommended as first-line medication treatment. However, up to 25% of preschool-age children with ADHD are treated with α2-adrenergic agonist medications, despite minimal evidence about their efficacy or adverse effects in this age range.
Objective: To determine the frequency of reported improvement in ADHD symptoms and adverse effects associated with α2-adrenergic agonists and stimulant medication for initial ADHD medication treatment in preschool-age children.
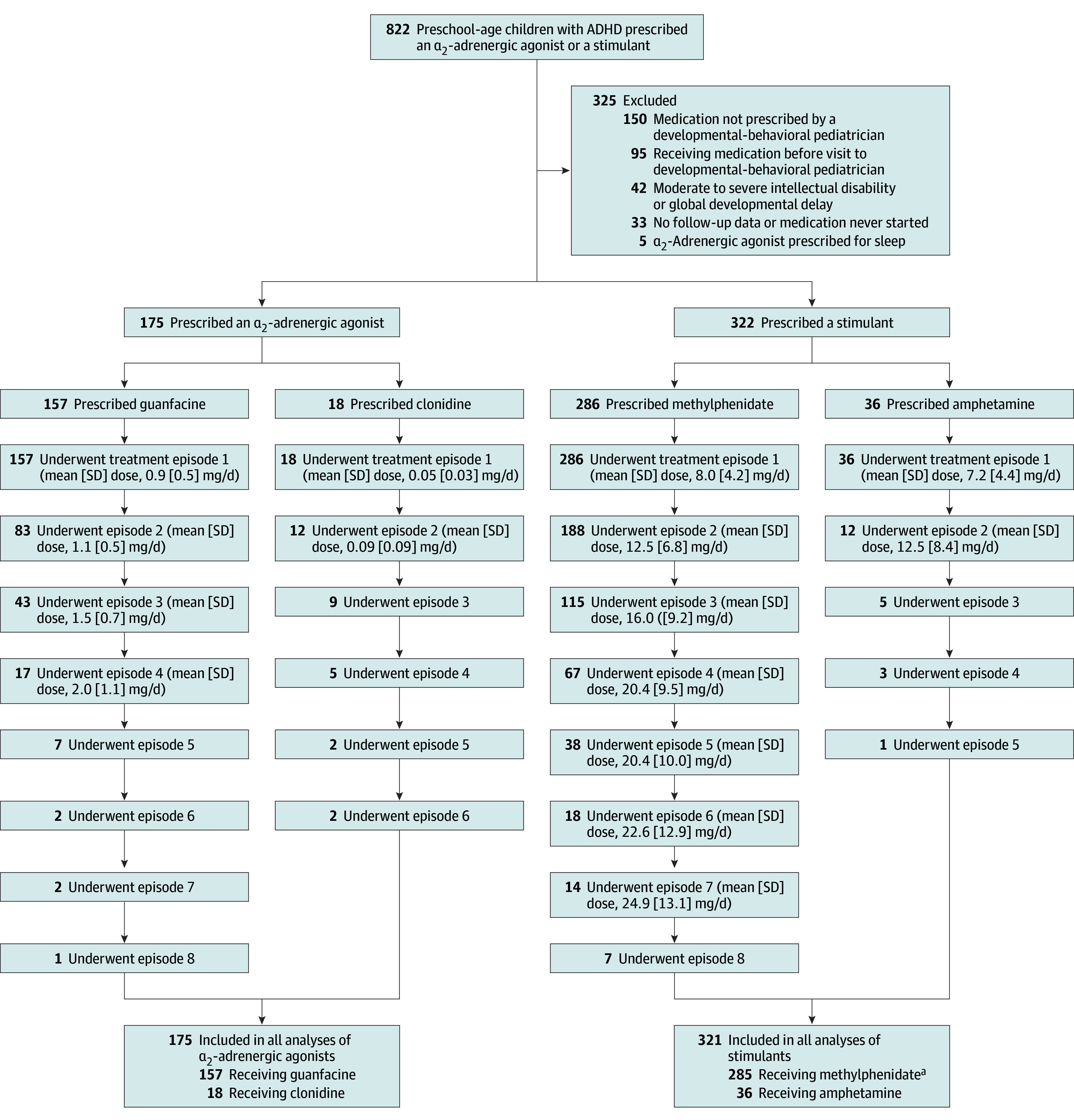
Design, setting, and participants: Retrospective electronic health record review. Data were obtained from health records of children seen at 7 outpatient developmental-behavioral pediatric practices in the Developmental Behavioral Pediatrics Research Network in the US. Data were abstracted for 497 consecutive children who were younger than 72 months when treatment with an α2-adrenergic agonist or stimulant medication was initiated by a developmental-behavioral pediatrician for ADHD and were treated between January 1, 2013, and July 1, 2017. Follow-up was complete on February 27, 2019.
Exposures: α2-Adrenergic agonist vs stimulant medication as initial ADHD medication treatment.
Main outcomes and measures: Reported improvement in ADHD symptoms and adverse effects.
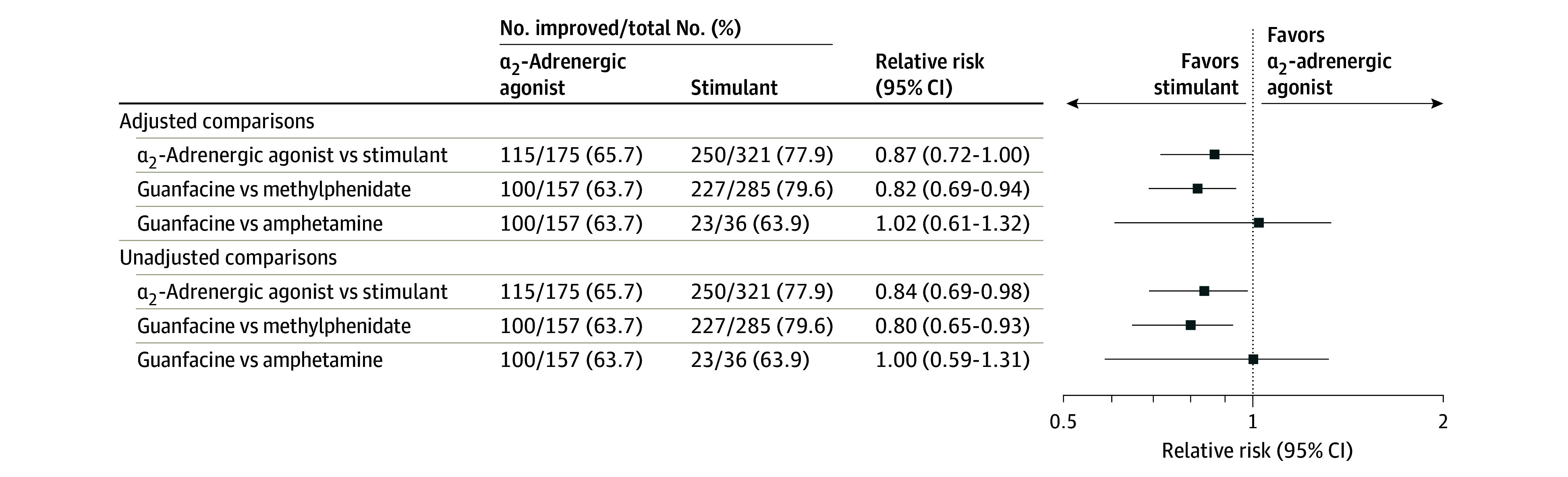
Results: Data were abstracted from electronic health records of 497 preschool-age children with ADHD receiving α2-adrenergic agonists or stimulants. Median child age was 62 months at ADHD medication initiation, and 409 children (82%) were males. For initial ADHD medication treatment, α2-adrenergic agonists were prescribed to 175 children (35%; median length of α2-adrenergic agonist use, 136 days) and stimulants were prescribed to 322 children (65%; median length of stimulant use, 133 days). Improvement was reported in 66% (95% CI, 57.5%-73.9%) of children who initiated α2-adrenergic agonists and 78% (95% CI, 72.4%-83.4%) of children who initiated stimulants. Only daytime sleepiness was more common for those receiving α2-adrenergic agonists vs stimulants (38% vs 3%); several adverse effects were reported more commonly for those receiving stimulants vs α2-adrenergic agonists, including moodiness/irritability (50% vs 29%), appetite suppression (38% vs 7%), and difficulty sleeping (21% vs 11%).
Conclusions and relevance: In this retrospective review of health records of preschool-age children with ADHD treated in developmental-behavioral pediatric practices, improvement was noted in the majority of children who received α2-adrenergic agonists or stimulants, with differing adverse effect profiles between medication classes. Further research, including from randomized clinical trials, is needed to assess comparative effectiveness of α2-adrenergic agonists vs stimulants.
Conflict of interest statement
Figures
Comment in
-
Comparison of Medication Treatments for Preschool Children With ADHD: A First Step Toward Addressing a Critical Gap.JAMA. 2021 May 25;325(20):2049-2050. doi: 10.1001/jama.2021.5603. JAMA. 2021. PMID: 33946095 No abstract available.
References
-
- Posner K, Melvin GA, Murray DW, et al. . Clinical presentation of attention-deficit/hyperactivity disorder in preschool children: the Preschoolers with Attention-Deficit/Hyperactivity Disorder Treatment Study (PATS). J Child Adolesc Psychopharmacol. 2007;17(5):547-562. doi:10.1089/cap.2007.0075 - DOI - PubMed
-
- Wolraich ML, Hagan JF Jr, Allan C, et al. ; Subcommittee on Children and Adolescents With Attention-Deficit/Hyperactive Disorder . Clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics. 2019;144(4):e20192528. doi:10.1542/peds.2019-2528 - DOI - PMC - PubMed
-
- Barbaresi WJ, Campbell L, Diekroger EA, et al. . Society for Developmental and Behavioral Pediatrics clinical practice guideline for the assessment and treatment of children and adolescents with complex attention-deficit/hyperactivity disorder. J Dev Behav Pediatr. 2020;41(suppl 2):s35-s57. doi:10.1097/DBP.0000000000000770 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
