

Immune-Mediated Disease Flares or New-Onset Disease in 27 Subjects Following mRNA/DNA SARS-CoV-2 Vaccination
- PMID: 33946748
- PMCID: PMC8146571
- DOI: 10.3390/vaccines9050435
Immune-Mediated Disease Flares or New-Onset Disease in 27 Subjects Following mRNA/DNA SARS-CoV-2 Vaccination
Abstract
Background: Infectious diseases and vaccines can occasionally cause new-onset or flare of immune-mediated diseases (IMDs). The adjuvanticity of the available SARS-CoV-2 vaccines is based on either TLR-7/8 or TLR-9 agonism, which is distinct from previous vaccines and is a common pathogenic mechanism in IMDs.
Methods: We evaluated IMD flares or new disease onset within 28-days of SARS-CoV-2 vaccination at five large tertiary centres in countries with early vaccination adoption, three in Israel, one in UK, and one in USA. We assessed the pattern of disease expression in terms of autoimmune, autoinflammatory, or mixed disease phenotype and organ system affected. We also evaluated outcomes.
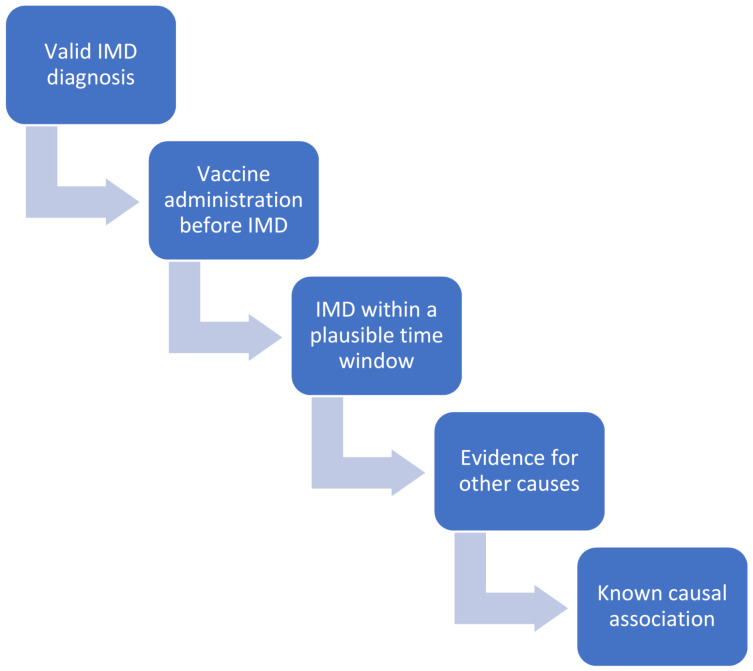
Findings: 27 cases included 17 flares and 10 new onset IMDs. 23/27 received the BNT - 162b2 vaccine, 2/27 the mRNA-1273 and 2/27 the ChAdOx1 vaccines. The mean age was 54.4 ± 19.2 years and 55% of cases were female. Among the 27 cases, 21 (78%) had at least one underlying autoimmune/rheumatic disease prior the vaccination. Among those patients with a flare or activation, four episodes occurred after receiving the second-dose and in one patient they occurred both after the first and the second-dose. In those patients with a new onset disease, two occurred after the second-dose and in one patient occurred both after the first (new onset) and second-dose (flare). For either dose, IMDs occurred on average 4 days later. Of the cases, 20/27 (75%) were mild to moderate in severity. Over 80% of cases had excellent resolution of inflammatory features, mostly with the use of corticosteroid therapy. Other immune-mediated conditions included idiopathic pericarditis (n = 2), neurosarcoidosis with small fiber neuropathy (n = 1), demyelination (n = 1), and myasthenia gravis (n = 2). In 22 cases (81.5%), the insurgence of Adverse event following immunization (AEFI)/IMD could not be explained based on the drug received by the patient. In 23 cases (85.2%), AEFI development could not be explained based on the underlying disease/co-morbidities. Only in one case (3.7%), the timing window of the insurgence of the side effect was considered not compatible with the time from vaccine to flare.
Interpretation: Despite the high population exposure in the regions served by these centers, IMDs flares or onset temporally-associated with SARS-CoV-2 vaccination appear rare. Most are moderate in severity and responsive to therapy although some severe flares occurred.
Funding: none.
Keywords: COVID-19; adenoviral vector-based vaccine; immune-mediated diseases; mRNA-based vaccine; vaccine safety.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Bonaccorsi G., Pierri F., Cinelli M., Flori A., Galeazzi A., Porcelli F., Schmidt A.L., Valensise C.M., Scala A., Quattrociocchi W., et al. Economic and social consequences of human mobility restrictions under COVID-19. Proc. Natl. Acad. Sci. USA. 2020;117:15530–15535. doi: 10.1073/pnas.2007658117. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
