

Advances in the Diagnosis and Treatment of Pediatric Acute Lymphoblastic Leukemia
- PMID: 33946897
- PMCID: PMC8124693
- DOI: 10.3390/jcm10091926
Advances in the Diagnosis and Treatment of Pediatric Acute Lymphoblastic Leukemia
Abstract
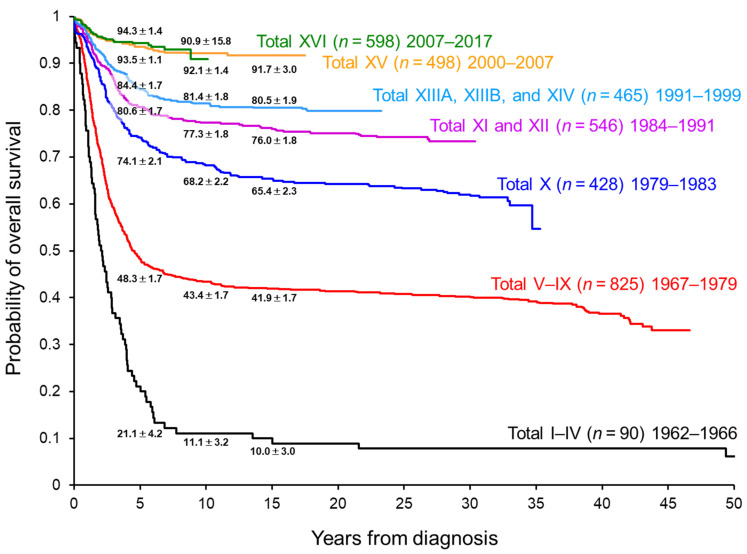
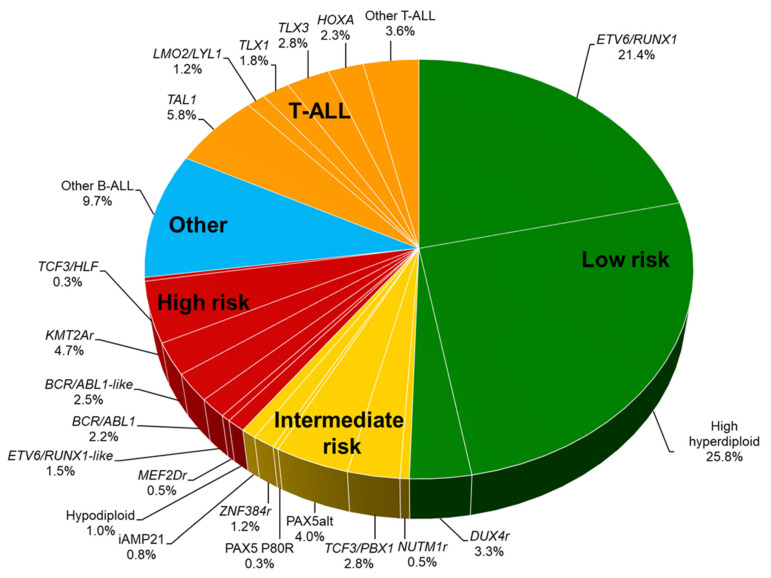
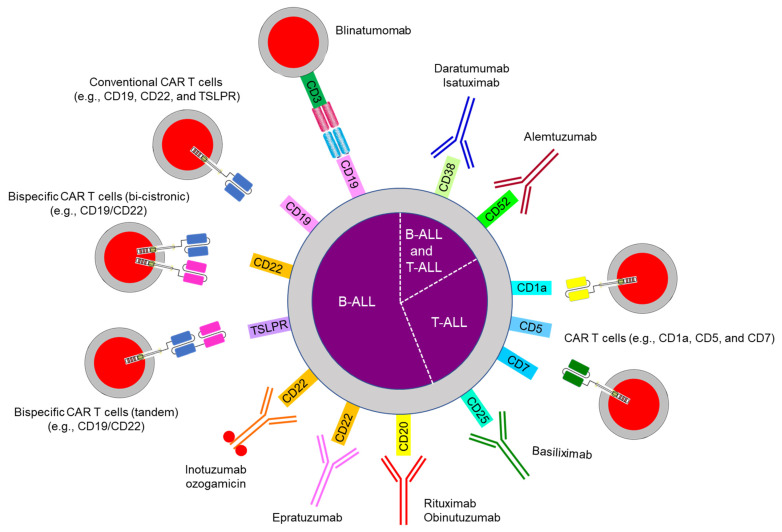
The outcomes of pediatric acute lymphoblastic leukemia (ALL) have improved remarkably during the last five decades. Such improvements were made possible by the incorporation of new diagnostic technologies, the effective administration of conventional chemotherapeutic agents, and the provision of better supportive care. With the 5-year survival rates now exceeding 90% in high-income countries, the goal for the next decade is to improve survival further toward 100% and to minimize treatment-related adverse effects. Based on genome-wide analyses, especially RNA-sequencing analyses, ALL can be classified into more than 20 B-lineage subtypes and more than 10 T-lineage subtypes with prognostic and therapeutic implications. Response to treatment is another critical prognostic factor, and detailed analysis of minimal residual disease can detect levels as low as one ALL cell among 1 million total cells. Such detailed analysis can facilitate the rational use of molecular targeted therapy and immunotherapy, which have emerged as new treatment strategies that can replace or reduce the use of conventional chemotherapy.
Keywords: acute lymphoblastic leukemia; advances; diagnosis; pediatric; treatment.
Conflict of interest statement
The authors have no conflict of interest, including specific financial interests, relationships, or affiliations relevant to the subject of this manuscript.
Figures
References
-
- National Cancer Institute Age-Adjusted and Age-Specific SEER Cancer Incidence Rates, 2014–2018. [(accessed on 18 April 2021)]; Available online: https://seer.cancer.gov/csr/1975_2018/results_merged/sect_02_childhood_c....
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
