

Phase III randomized study of carboplatin pemetrexed with or without bevacizumab with initial versus "at progression" cerebral radiotherapy in advanced non squamous non-small cell lung cancer with asymptomatic brain metastasis
- PMID: 33948123
- PMCID: PMC8053829
- DOI: 10.1177/17588359211006983
Phase III randomized study of carboplatin pemetrexed with or without bevacizumab with initial versus "at progression" cerebral radiotherapy in advanced non squamous non-small cell lung cancer with asymptomatic brain metastasis
Abstract
Background: The role and timing of whole or stereotaxic brain radiotherapy (BR) in patients with advanced non-small cell lung cancer (aNSCLC) and asymptomatic brain metastases (aBMs) are not well established. This study investigates whether deferring BR until cerebral progression was superior to upfront BR for patients with aNSCLC and aBM.
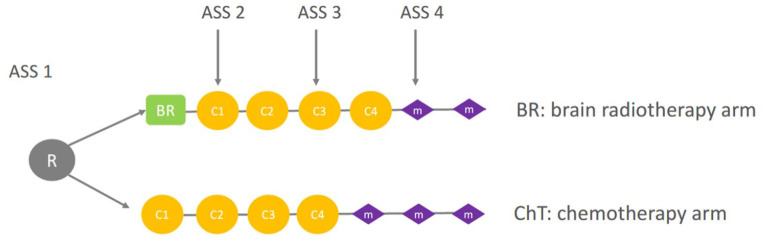
Methods: This open-label, multicenter, phase III trial, randomized (1:1) aNSCLC patients with aBMs to receive upfront BR and chemotherapy: platin-pemetrexed and bevacizumab in eligible patients, followed by maintenance pemetrexed with or without bevacizumab, BR arm, or the same chemotherapy with BR only at cerebral progression, chemotherapy (ChT) arm. Primary endpoint was progression-free survival (PFS), secondary endpoints were overall survival (OS), global, extra-cerebral and cerebral objective response rate (ORR), toxicity, and quality of life [ClinicalTrials.gov identifier: NCT02162537].
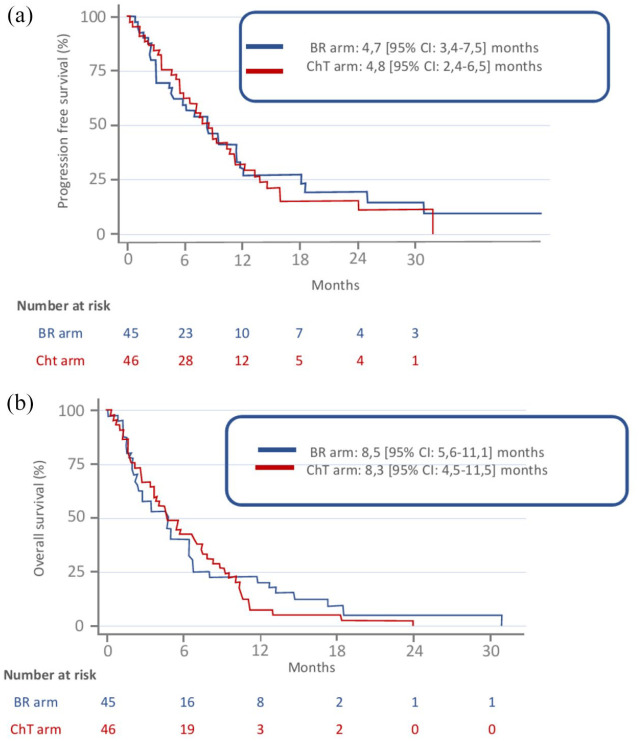
Results: The trial was stopped early because of slow recruitment. Among 95 included patients, 91 were randomized in 24 centers: 45 to BR and 46 to ChT arms (age: 60 ± 8.1, men: 79%, PS 0/1: 51.7%/48.3%; adenocarcinomas: 92.2%, extra-cerebral metastases: 57.8%, without differences between arms.) Significantly more patients in the BR-arm received BR compare with those in the ChT arm (87% versus 20%; p < 0.001); there were no significant differences between BR and ChT arms for median PFS: 4.7, 95% confidence interval (CI):3.4-7.5 versus 4.8, 95% CI: 2.4-6.5 months, for median OS: 8.5, 95% CI:.6-11.1 versus 8.3, 95% CI:4.5-11.5 months, cerebral and extra-cerebral ORR (27% versus 13%, p = 0.064, and 30% versus 41%, p = 0.245, respectively). The ChT arm had more grade 3/4 neutropenia than the BR arm (13% versus 6%, p = 0.045); others toxicities were comparable.
Conclusion: The significant BR rate difference between the two arms suggests that upfront BR is not mandatory in aNSCLC with aBM but this trial failed to show that deferring BR for aBM is superior in terms of PFS from upfront BR.
Keywords: bevacizumab; cerebral metastasis; management; non-small–cell lung cancer; pemetrexed; radiotherapy.
© The Author(s), 2021.
Conflict of interest statement
Conflict of interest statement: The authors declare that there is no conflict of interest.
Figures
References
-
- Barnholtz-Sloan JS, Sloan AE, Davis FG, et al.. Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J Clin Oncol 2004; 22: 2865–2872. - PubMed
-
- Peters S, Bexelius C, Munk V, et al.. The impact of brain metastasis on quality of life, resource utilization and survival in patients with non-small-cell lung cancer. Cancer Treat Rev 2016; 45: 139–162. - PubMed
-
- Levy A, Faivre-Finn C, Hasan B, et al.. Diversity of brain metastases screening and management in non-small cell lung cancer in Europe: results of the European Organisation for research and treatment of Cancer Lung Cancer Group survey. Eur J Cancer 2018; 93: 37–46. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
