

Temporal muscle thickness and area are an independent prognostic factors in patients aged 75 or younger with aneurysmal subarachnoid hemorrhage treated by clipping
- PMID: 33948321
- PMCID: PMC8088495
- DOI: 10.25259/SNI_814_2020
Temporal muscle thickness and area are an independent prognostic factors in patients aged 75 or younger with aneurysmal subarachnoid hemorrhage treated by clipping
Abstract
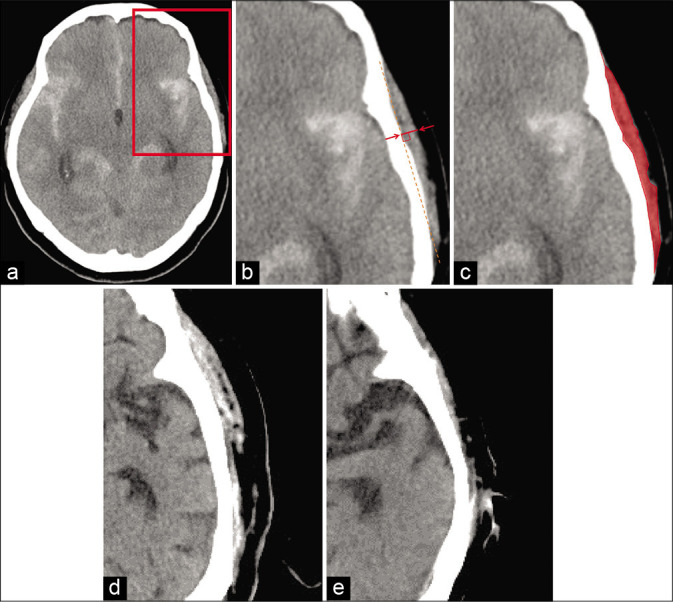
Background: Skeletal muscle mass is an important factor for various diseases' outcomes. As for its indicators, temporal muscle thickness (TMT) and temporal muscle area (TMA) on the head computed tomography are useful, and TMT and TMA were reported as potential prognostic factors for aneurysmal subarachnoid hemorrhage (SAH). We examined the clinical characteristics, including TMT and TMA, of SAH patients aged 75 or younger.
Methods: We retrospectively investigated 127 SAH patients with all World Federation of Neurosurgical Societies (WFNS) grades and treated by clipping between 2009 and 2019. Clinical outcome was measured with the modified Rankin Scale (mRS) at 6 months, with favorable outcome defined as mRS 0-2. The associations between the clinical variables and the outcomes were analyzed.
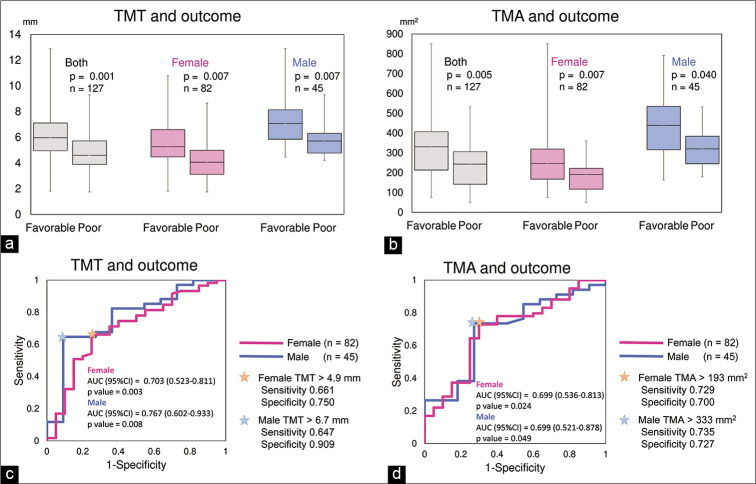
Results: The mean age was 60.6 (32-74) years, and 65% were women. The mean ± standard deviation of WFNS grade was 2.8 ± 1.4. TMT and TMA were larger in the favorable outcome group than the poor one. Multivariate analysis revealed that age, smoking, WFNS grade, and TMT or TMA were associated with favorable outcome. Receiver operating characteristic analysis found that the threshold of TMT was 4.9 mm in female and 6.7 mm in male, and that of TMA was 193 mm2 in female and 333 mm2 in male.
Conclusion: The odds ratios for TMT and TMA related to clinical outcome were lower than for smoking and WFNS grade; however, on multivariate analysis they remained independent prognostic factors in SAH patients aged 75 or younger treated by clipping. Further studies are needed to confirm these findings.
Keywords: Cerebral aneurysm; Clipping; Prognostic factor; Sarcopenia; Subarachnoid hemorrhage; Temporal muscle thickness and area.
Copyright: © 2021 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Clinical characteristics of aneurysmal subarachnoid hemorrhage in the elderly over 75; would temporal muscle be a potential prognostic factor as an indicator of sarcopenia?Clin Neurol Neurosurg. 2019 Nov;186:105535. doi: 10.1016/j.clineuro.2019.105535. Epub 2019 Sep 23. Clin Neurol Neurosurg. 2019. PMID: 31569058
-
Initial Temporal Muscle Thickness and Area: Poor Predictors of Neurological Outcome in Aneurysmal Subarachnoid Hemorrhage in a Central European Patient Cohort.J Clin Med. 2023 Aug 10;12(16):5210. doi: 10.3390/jcm12165210. J Clin Med. 2023. PMID: 37629252 Free PMC article.
-
Temporal Muscle as an Indicator of Sarcopenia is Independently Associated with Hunt and Kosnik Grade on Admission and the Modified Rankin Scale Score at 6 Months of Patients with Subarachnoid Hemorrhage Treated by Endovascular Coiling.World Neurosurg. 2020 May;137:e526-e534. doi: 10.1016/j.wneu.2020.02.033. Epub 2020 Feb 14. World Neurosurg. 2020. PMID: 32061954
-
Effect of statin treatment on vasospasm-related morbidity and functional outcome in patients with aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis.J Neurosurg. 2017 Aug;127(2):291-301. doi: 10.3171/2016.5.JNS152900. Epub 2016 Oct 7. J Neurosurg. 2017. PMID: 27715439
-
Neuropsychological function after endovascular and neurosurgical treatment of subarachnoid hemorrhage: a systematic review and meta-analysis.J Neurosurg. 2018 Mar;128(3):768-776. doi: 10.3171/2016.11.JNS162055. Epub 2017 Apr 14. J Neurosurg. 2018. PMID: 28409729
Cited by
-
Age- and sex-adjusted CT-based reference values for temporal muscle thickness, cross-sectional area and radiodensity.Sci Rep. 2025 Jan 18;15(1):2393. doi: 10.1038/s41598-025-86711-7. Sci Rep. 2025. PMID: 39827306 Free PMC article.
-
Author's Reply to "Painting a Clearer Picture by Measuring the Quadriceps Muscle with Ultrasound".Gerontology. 2024;70(11):1150-1151. doi: 10.1159/000540996. Epub 2024 Aug 27. Gerontology. 2024. PMID: 39191208 Free PMC article. No abstract available.
-
Correlation between temporal muscle thickness and grip strength in hemiplegic patients with acute stroke.Front Neurol. 2023 Nov 23;14:1252707. doi: 10.3389/fneur.2023.1252707. eCollection 2023. Front Neurol. 2023. PMID: 38073618 Free PMC article.
-
Temporal Muscle and Stroke-A Narrative Review on Current Meaning and Clinical Applications of Temporal Muscle Thickness, Area, and Volume.Nutrients. 2022 Feb 6;14(3):687. doi: 10.3390/nu14030687. Nutrients. 2022. PMID: 35277046 Free PMC article. Review.
-
Oral health and temporal muscle thickness.Surg Neurol Int. 2021 Oct 19;12:527. doi: 10.25259/SNI_905_2021. eCollection 2021. Surg Neurol Int. 2021. PMID: 34754577 Free PMC article. No abstract available.
References
-
- Bayram S, Akgül T, Adıyaman AE, Karalar Ş Dölen D, Aydoseli A. Effect of sarcopenia on mortality after percutaneous vertebral augmentation treatment for osteoporotic vertebral compression fractures in elderly patients: A retrospective cohort study. World Neurosurg. 2020;138:e354–60. - PubMed
-
- Benatti FB, Pedersen BK. Exercise as an anti-inflammatory therapy for rheumatic diseases-myokine regulation. Nat Rev Rheumatol. 2015;11:86–97. - PubMed
-
- Binay Safer V, Safer U. Comment on. “Clinical characteristics of aneurysmal subarachnoid hemorrhage (SAH) in the elderly over 75: Would temporal muscle be a potential prognostic factor as an indicator of sarcopenia? ” Clin Neurol Neurosurg. 2020;188:105600. - PubMed
-
- Chen LK, Liu LK, Woo J, Assantachai P, Auyeung TW, Bahyah KS, et al. Sarcopenia in Asia: Consensus report of the Asian working group for sarcopenia. J Am Med Dir Assoc. 2014;15:95–101. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials