

COVID-19 Related Acute Hemorrhagic Necrotizing Encephalitis: A Report of Two Cases and Literature Review
- PMID: 33948421
- PMCID: PMC8087949
- DOI: 10.7759/cureus.14236
COVID-19 Related Acute Hemorrhagic Necrotizing Encephalitis: A Report of Two Cases and Literature Review
Abstract
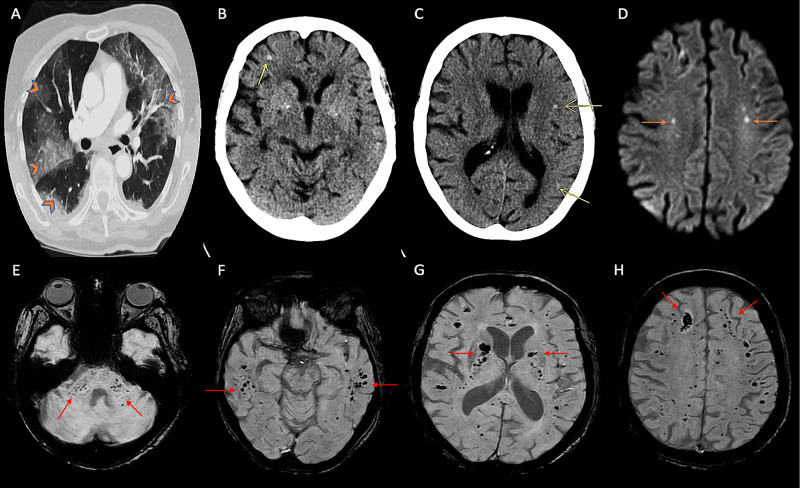
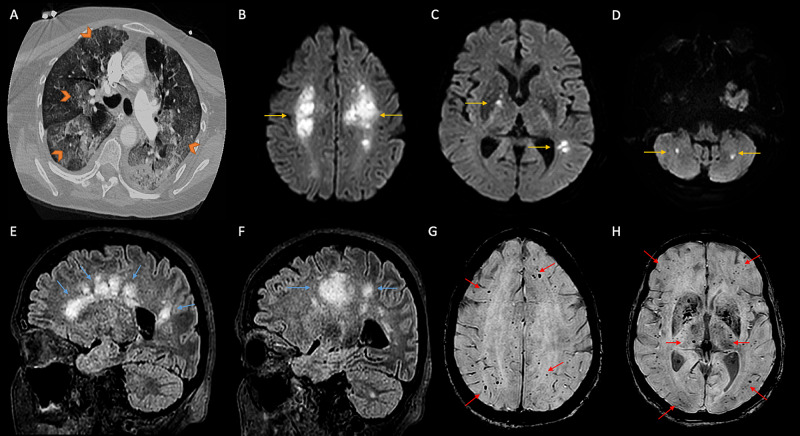
Coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), a novel coronavirus, has proven neurotropism and causes a multitude of neurologic manifestations. Acute hemorrhagic necrotizing encephalitis (AHNE), though rare, can be seen in patients with severe infection and is associated with devastating neurologic outcomes. The true prevalence of this syndrome is unknown due to underrecognition, difficulty in timely acquisition of neuroimaging, and high mortality in this subset of patients escaping detection. It is a distinct clinicoradiological syndrome, with patients suffering from rapidly worsening encephalopathy and coma within the first two weeks of severe illness and hemorrhagic necrotizing parenchymal changes on neuroimaging. The pathophysiology of this syndrome is unclear but hypothesized to occur due to cytokine storm, blood-brain-barrier dysfunction, and direct viral-mediated endotheliopathy. Diagnosis requires a high index of suspicion in patients who have unexplained persistent severe encephalopathy associated with COVID-19 infection. Most patients have elevated systemic inflammatory markers and severe lung disease with hypoxic respiratory failure requiring mechanical ventilation. MRI is the imaging modality of choice, with a distinct neuroimaging pattern. CSF (cerebrospinal fluid) studies have a low yield for viral particle detection with currently available testing. While long-term outcomes are unclear, early immunomodulatory treatment with intravenous immunoglobulin, plasma exchange, and steroids may portend a favorable outcome. We discuss two cases of COVID-19 related AHNE and also include a pertinent literature search of similar cases in PubMed to consolidate the AHNE clinical syndrome, neuroimaging characteristics, management strategies, and reported short-term prognosis.
Keywords: acute hemorrhagic necrotizing encephalitis; cerebral microhemorrhage; covid-19; cytokine release storm; dexamethasone convalescent plasma; disorder of consciousness; remdesivir; sars-cov-2 (severe acute respiratory syndrome coronavirus -2).
Copyright © 2021, Mullaguri et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
SARS-CoV-2-Associated Acute Hemorrhagic, Necrotizing Encephalitis (AHNE) Presenting with Cognitive Impairment in a 44-Year-Old Woman without Comorbidities: A Case Report.Am J Case Rep. 2020 Aug 16;21:e925641. doi: 10.12659/AJCR.925641. Am J Case Rep. 2020. PMID: 32799213 Free PMC article.
-
COVID-19 and neuroinflammation: a literature review of relevant neuroimaging and CSF markers in central nervous system inflammatory disorders from SARS-COV2.J Neurol. 2021 Dec;268(12):4448-4478. doi: 10.1007/s00415-021-10611-9. Epub 2021 May 19. J Neurol. 2021. PMID: 34009454 Free PMC article. Review.
-
Neurological manifestations of COVID-19 and other coronaviruses: A systematic review.Neurol Psychiatry Brain Res. 2020 Sep;37:27-32. doi: 10.1016/j.npbr.2020.05.008. Epub 2020 May 31. Neurol Psychiatry Brain Res. 2020. PMID: 32834527 Free PMC article. Review.
-
Encephalopathy in COVID-19 Patients.Cureus. 2021 Jul 25;13(7):e16620. doi: 10.7759/cureus.16620. eCollection 2021 Jul. Cureus. 2021. PMID: 34458032 Free PMC article.
-
Spectrum of Neurological Manifestations in Covid-19: A Review.Neurol India. 2020 May-Jun;68(3):560-572. doi: 10.4103/0028-3886.289000. Neurol India. 2020. PMID: 32643664 Review.
Cited by
-
COVID-19-Associated Encephalopathy-Case Series and Clinical Considerations.J Clin Med. 2022 Feb 13;11(4):981. doi: 10.3390/jcm11040981. J Clin Med. 2022. PMID: 35207253 Free PMC article.
-
COVID-19 related acute necrotizing encephalopathy with extremely high interleukin-6 and RANBP2 mutation in a patient with recently immunized inactivated virus vaccine and no pulmonary involvement.BMC Infect Dis. 2022 Jul 23;22(1):640. doi: 10.1186/s12879-022-07610-0. BMC Infect Dis. 2022. PMID: 35870896 Free PMC article.
-
Coronavirus or Cholangitis? An Acute Necrotizing Encephalopathy Caused by COVID-19.Cureus. 2023 Aug 31;15(8):e44448. doi: 10.7759/cureus.44448. eCollection 2023 Aug. Cureus. 2023. PMID: 37791164 Free PMC article.
-
Network Analysis of Neurobehavioral Symptom Patterns in an International Sample of Spanish-Speakers with a History of COVID-19 and Controls.Int J Environ Res Public Health. 2022 Dec 23;20(1):183. doi: 10.3390/ijerph20010183. Int J Environ Res Public Health. 2022. PMID: 36612505 Free PMC article.
-
A case of successive development of possible acute necrotizing encephalopathy after COVID-19 pneumonia.SAGE Open Med Case Rep. 2022 Mar 15;10:2050313X221083653. doi: 10.1177/2050313X221083653. eCollection 2022. SAGE Open Med Case Rep. 2022. PMID: 35308052 Free PMC article.
References
-
- Evidence of the COVID-19 virus targeting the CNS: tissue distribution, host-virus interaction, and proposed neurotropic mechanisms. Baig AM, Khaleeq A, Ali U, Syeda H. ACS Chem Neurosci. 2020;11:995–998. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous