

This is a preprint.
When can we stop wearing masks? Agent-based modeling to identify when vaccine coverage makes nonpharmaceutical interventions for reducing SARS-CoV-2 infections redundant in indoor gatherings
- PMID: 33948613
- PMCID: PMC8095232
- DOI: 10.1101/2021.04.19.21255737
When can we stop wearing masks? Agent-based modeling to identify when vaccine coverage makes nonpharmaceutical interventions for reducing SARS-CoV-2 infections redundant in indoor gatherings
Abstract
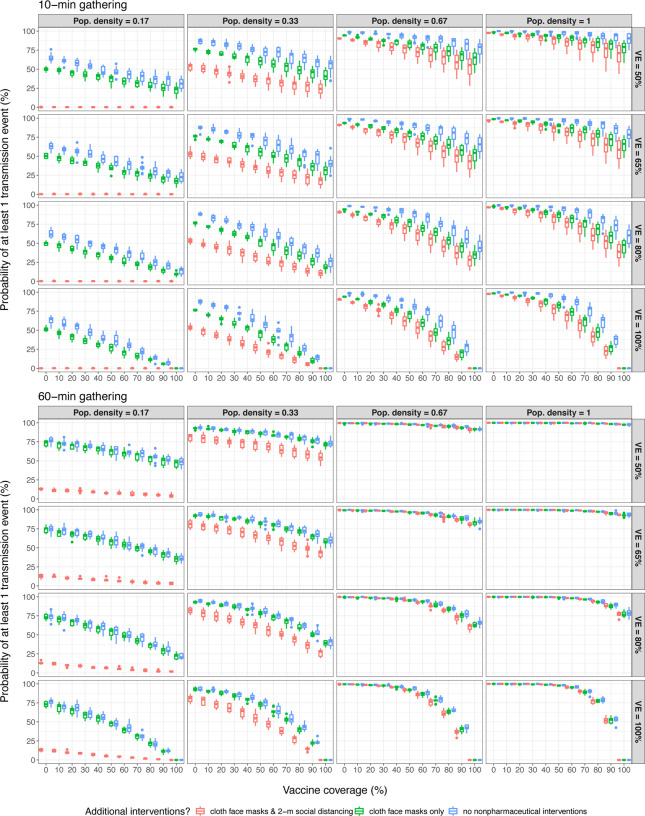
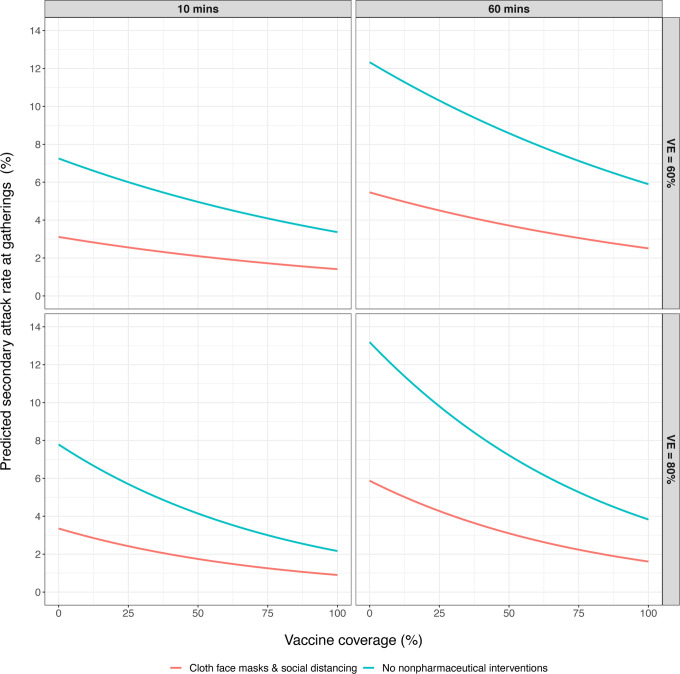
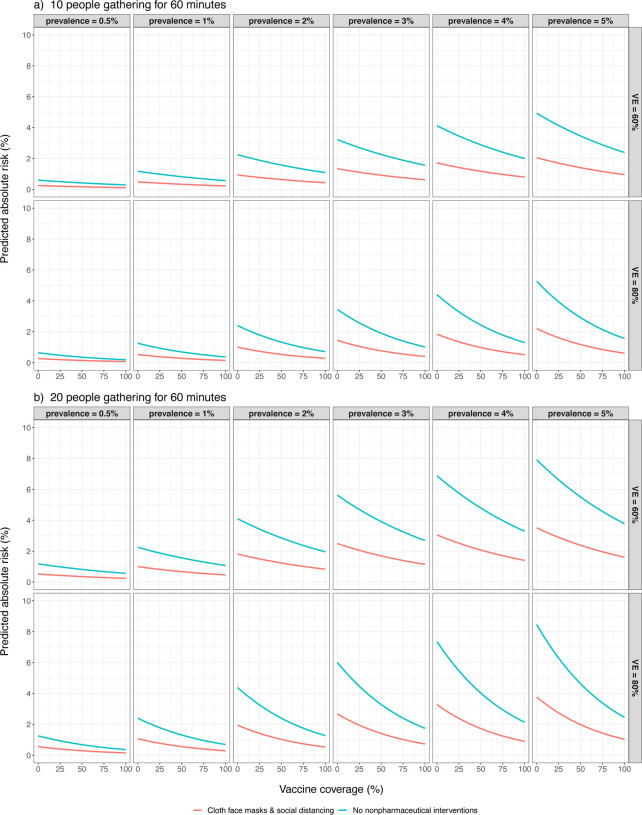
As vaccination efforts to combat the COVID-19 pandemic are ramping up worldwide, there are rising concerns that individuals will begin to eschew nonpharmaceutical interventions for preventing SARS-CoV-2 transmission and attempt to return to pre-pandemic normalcy before vaccine coverage levels effectively mitigate transmission risk. In the U.S.A., some governing bodies have already weakened or repealed guidelines for nonpharmaceutical intervention use, despite a recent spike in national COVID-19 cases and majority population of unvaccinated individuals. Recent modeling suggests that repealing nonpharmaceutical intervention guidelines too early into vaccine rollouts will lead to localized increases in COVID-19 cases, but the magnitude of nonpharmaceutical intervention effects on individual-level SARS-CoV-2 infection risk in fully- and partially-vaccinated populations is unclear. We use a previously-published agent-based model to simulate SARS-CoV-2 transmission in indoor gatherings of varying durations, population densities, and vaccination coverage levels. By simulating nonpharmaceutical interventions in some gatherings but not others, we were able to quantify the difference in SARS-CoV-2 infection risk when nonpharmaceutical interventions were used, relative to scenarios with no nonpharmaceutical interventions. We found that nonpharmaceutical interventions will often reduce secondary attack rates, especially during brief interactions, and therefore there is no definitive vaccination coverage level that makes nonpharmaceutical interventions completely redundant. However, the reduction effect on absolute SARS-CoV-2 infection risk conferred by nonpharmaceutical interventions is likely proportional to COVID-19 prevalence. Therefore, if COVID-19 prevalence decreases in the future, nonpharmaceutical interventions will likely still confer protective effects but potential benefits may be small enough to remain within "effectively negligible" risk thresholds.
Keywords: COVID-19; SARS-CoV-2; agent-based model; indoor transmission; nonpharmaceutical interventions; vaccine.
Conflict of interest statement
Declarations of Interest: None
Figures

Similar articles
-
Association of Simulated COVID-19 Vaccination and Nonpharmaceutical Interventions With Infections, Hospitalizations, and Mortality.JAMA Netw Open. 2021 Jun 1;4(6):e2110782. doi: 10.1001/jamanetworkopen.2021.10782. JAMA Netw Open. 2021. PMID: 34061203 Free PMC article.
-
The Impact of Vaccination to Control COVID-19 Burden in the United States: A Simulation Modeling Approach.medRxiv [Preprint]. 2021 Mar 31:2021.03.22.21254131. doi: 10.1101/2021.03.22.21254131. medRxiv. 2021. Update in: PLoS One. 2021 Jul 14;16(7):e0254456. doi: 10.1371/journal.pone.0254456. PMID: 33791738 Free PMC article. Updated. Preprint.
-
The impact of vaccination to control COVID-19 burden in the United States: A simulation modeling approach.PLoS One. 2021 Jul 14;16(7):e0254456. doi: 10.1371/journal.pone.0254456. eCollection 2021. PLoS One. 2021. PMID: 34260633 Free PMC article.
-
Nonpharmaceutical public health interventions to curb the COVID-19 pandemic: a narrative review.J Infect Dev Ctries. 2022 Apr 30;16(4):583-591. doi: 10.3855/jidc.14580. J Infect Dev Ctries. 2022. PMID: 35544617 Review.
-
Physical interventions to interrupt or reduce the spread of respiratory viruses.Cochrane Database Syst Rev. 2020 Nov 20;11(11):CD006207. doi: 10.1002/14651858.CD006207.pub5. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2023 Jan 30;1:CD006207. doi: 10.1002/14651858.CD006207.pub6. PMID: 33215698 Free PMC article. Updated.
References
-
- Adams WC. Measurement of breathing rate and volume in routinely performed daily activities. 1993. Final Report, Contract No. A033–205. California Air Resources Board, Sacramento, CA, USA. https://ww2.arb.ca.gov/sites/default/files/classic//research/apr/past/a0....
-
- Applewhite A, Stancampiano FF, Harris DM, Manaois A, Dimuna J, Glenn J, Heckman MG, Brushaber DE, Sher T, & Valery JR. (2020). A retrospective analysis of gender-based difference in adherence to influenza vaccination during the 2018–2019 season. J Prim Care & Commun Heal 11:1–6. 10.1177/2150132720958532. - DOI - PMC - PubMed
-
- Castillo JE, & Weibel JA. (2018). A point sink superposition method for predicting droplet interaction effects during vapor-diffusion-driven dropwise condensation in humid air. Int J Heat Mass Trans 118:708–719. 10.1016/j.ijheatmasstransfer.2017.11.045 - DOI
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous