

Using gastrointestinal distress reports to predict youth anxiety risk: Implications for mental health literacy and community care
- PMID: 33948944
- PMCID: PMC11804969
- DOI: 10.1002/dev.22126
Using gastrointestinal distress reports to predict youth anxiety risk: Implications for mental health literacy and community care
Abstract
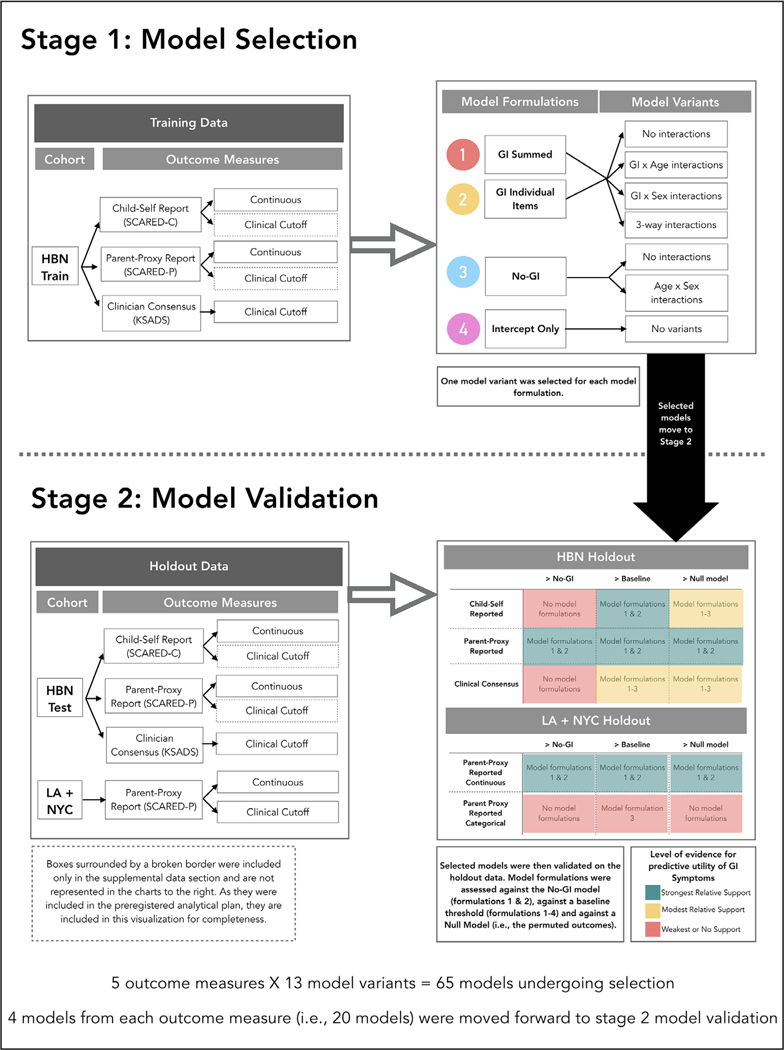
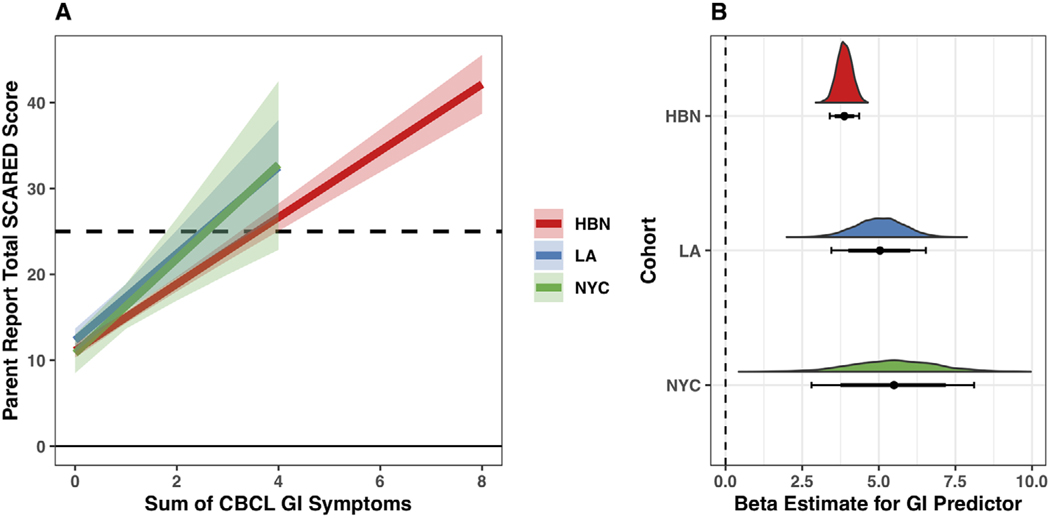
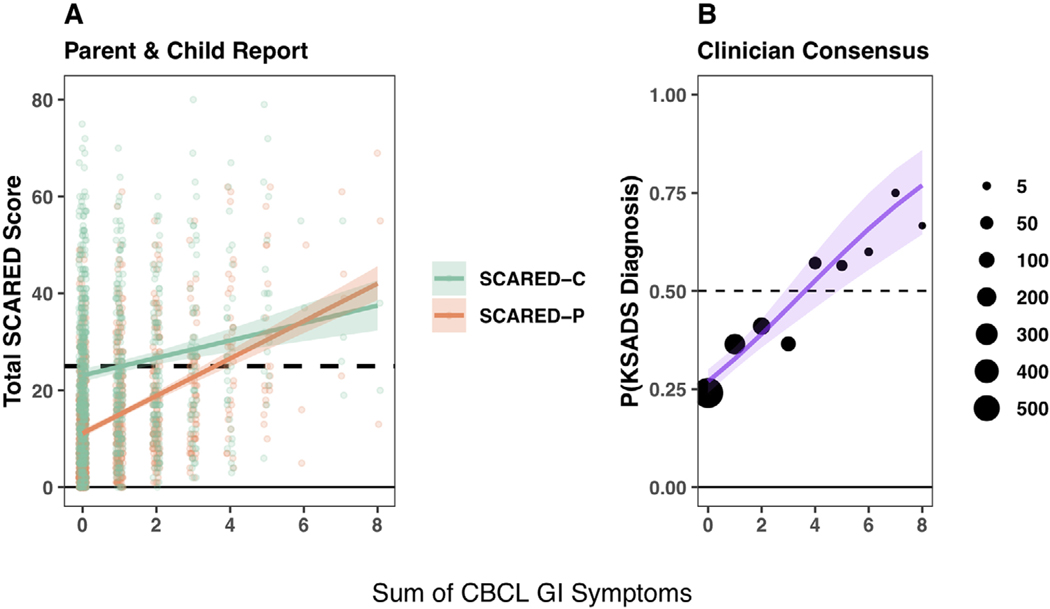
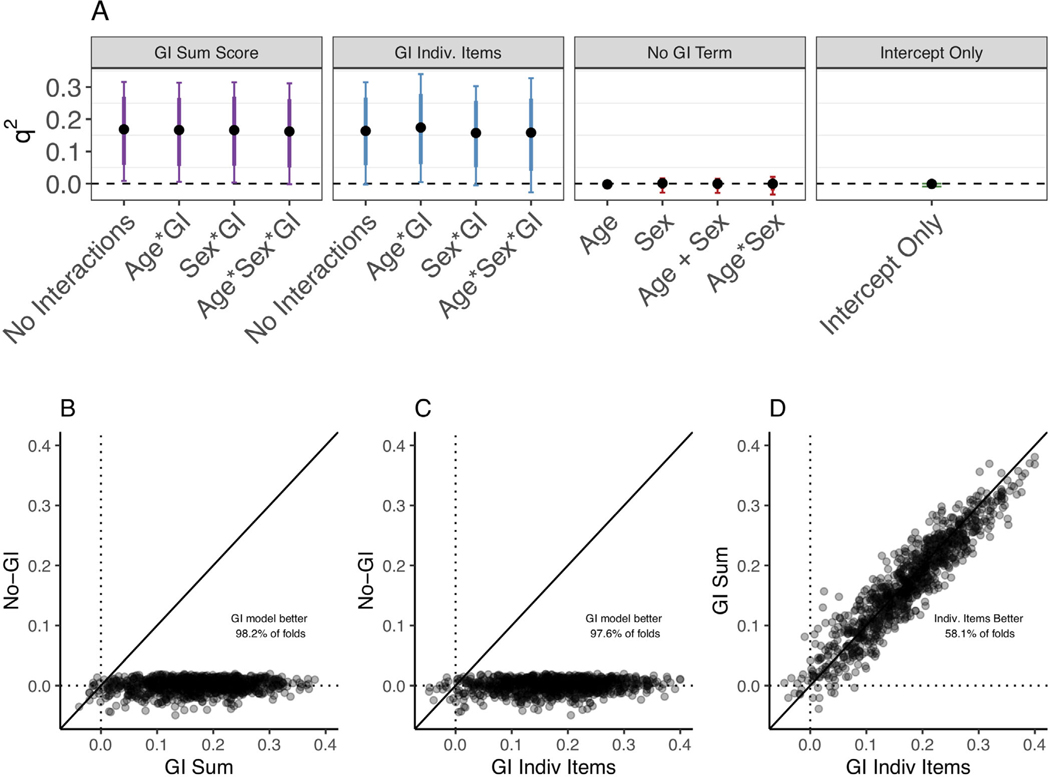
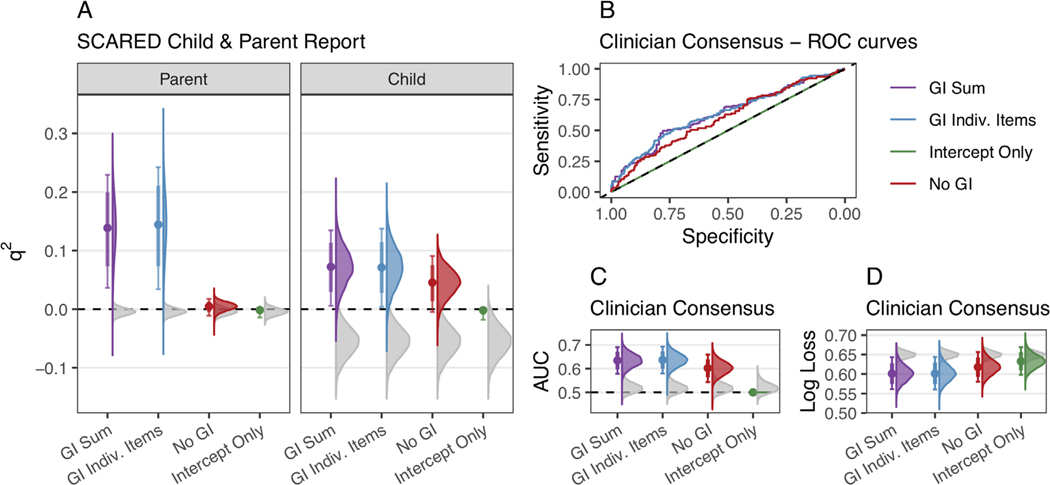
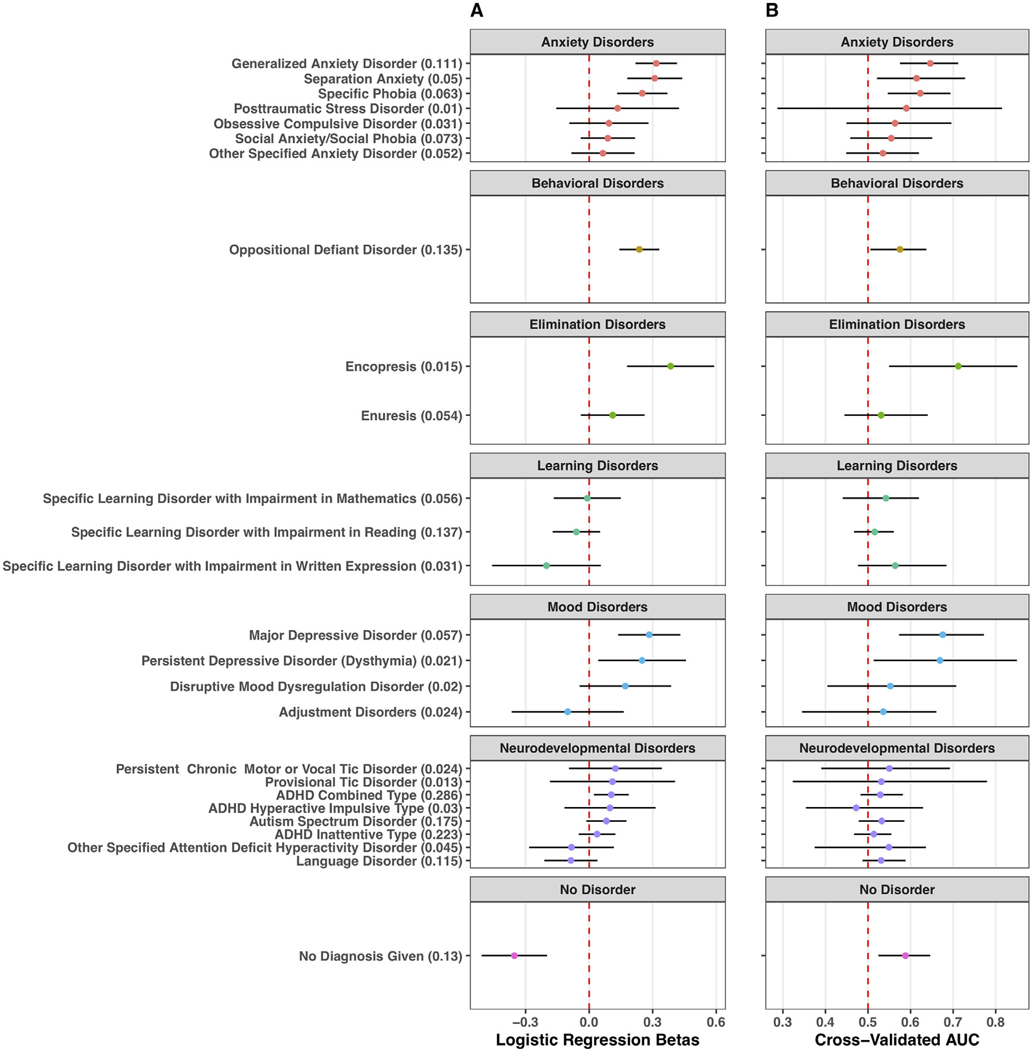
This study investigates the generalizability and predictive validity of associations between gastrointestinal (GI) symptoms and youth anxiety to establish their utility in community mental health decision-making. We analyzed data from youth ages 3 to 21 years in volunteer cohorts collected in Los Angeles (N = 327) and New York City (N = 102), as well as the Healthy Brain Network cohort (N = 1957). Youth GI distress was measured through items taken from the parent-reported Child Behavior Checklist (CBCL). We examined generalizability of GI-anxiety associations across cohorts and anxiety reporters, then evaluated the performance of these models in predicting youth anxiety in holdout data. Consistent with previous work, higher levels of gastrointestinal distress were associated with more parent-reported youth anxiety behaviors in all three cohorts. Models trained on data from the Healthy Brain Network cohort predicted parent-reported and child-reported anxiety behaviors, as well as clinician-evaluated anxiety diagnoses, at above chance levels in holdout data. Models which included GI symptoms often, but not always, outperformed models based on age and sex alone in predicting youth anxiety. Based on the generalizability and predictive validity of GI-anxiety associations investigated here, GI symptoms may be an effective tool for child-facing professionals for identifying children at risk for anxiety (Preprint: https://psyarxiv.com/zgavu/).
Keywords: anxiety; gastrointestinal; prediction; replication; youth.
© 2021 Wiley Periodicals LLC.
Conflict of interest statement
CONFLICT OF INTEREST
The authors declare no conflict of interest.
Figures
References
-
- Achenbach TM (1991). Integrative guide for the 1991 CBCL/4–18, Ysr, and Trf profiles (1st US-1st Printing ed.). Department of Psychiatry, University of Vermont.
-
- Achenbach TM, & Edelbrock CS (1983). Manual for the child behavior checklist and revised child behavior profile. Department of Psychiatry, University of Vermont.
-
- Alegria M, Shrout PE, Canino G, Alvarez K, Wang Y, Bird H, Markle SL, Ramos-Olazagasti M, Rivera DV, Cook BL, Musa GJ, Falgas-Bague I, NeMoyer A, Dominique G, & Duarte C. (2019). The effect of minority status and social context on the development of depression and anxiety: A longitudinal study of Puerto Rican descent youth. World Psychiatry, 18(3), 298–307. 10.1002/wps.20671 - DOI - PMC - PubMed
-
- Alexander LM, Escalera J, Ai L, Andreotti C, Febre K, Mangone A, Vega-Potler N, Langer N, Alexander A, Kovacs M, Litke S, O’Hagan B, Andersen J, Bronstein B, Bui A, Bushey M, Butler H, Castagna V, Camacho N, ..., Milham MP (2017). An open resource for transdiagnostic research in pediatric mental health and learning disorders. Scientific Data, 4, 170181. 10.1038/sdata.2017.181 - DOI - PMC - PubMed
-
- Ambekar A, Ward C, Mohammed J, Male S, & Skiena S. (2009). Name-ethnicity classification from open sources. Proceedings of the 15th ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, USA, 49–58. 10.1145/1557019.1557032 - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
