

A calibration CT mini-lung-phantom created by 3-D printing and subtractive manufacturing
- PMID: 33949078
- PMCID: PMC8200432
- DOI: 10.1002/acm2.13263
A calibration CT mini-lung-phantom created by 3-D printing and subtractive manufacturing
Abstract
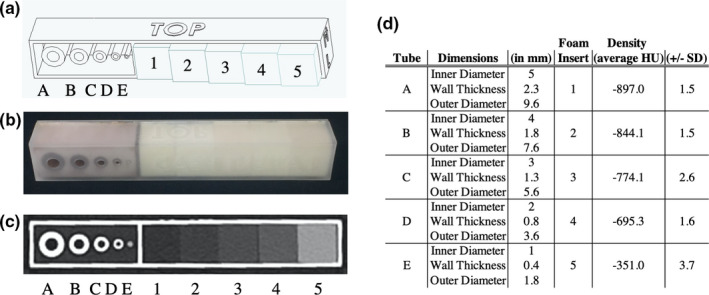
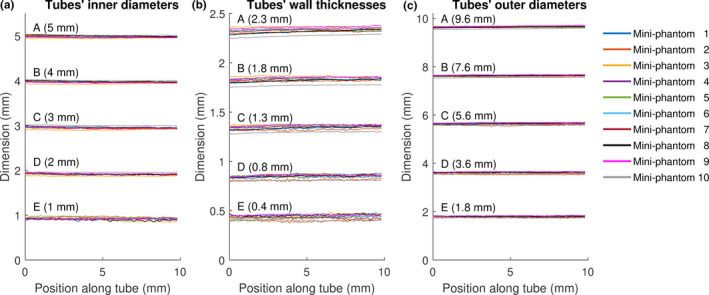
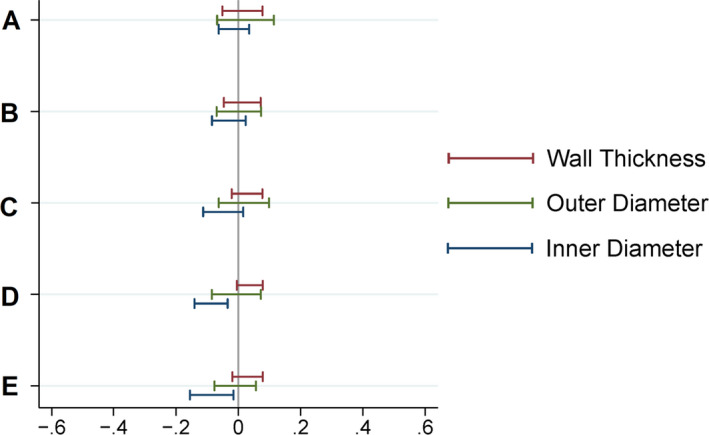
We describe the creation and characterization of a calibration CT mini-lung-phantom incorporating simulated airways and ground-glass densities. Ten duplicate mini-lung-phantoms with Three-Dimensional (3-D) printed tubes simulating airways and gradated density polyurethane foam blocks were designed and built. Dimensional accuracy and CT numbers were measured using micro-CT and clinical CT scanners. Micro-CT images of airway tubes demonstrated an average dimensional variation of 0.038 mm from nominal values. The five different densities of incorporated foam blocks, simulating ground-glass, showed mean CT numbers (±standard deviation) of -897.0 ± 1.5, -844.1 ± 1.5, -774.1 ± 2.6, -695.3 ± 1.6, and -351.0 ± 3.7 HU, respectively. Three-Dimensional printing and subtractive manufacturing enabled rapid, cost-effective production of ground-truth calibration mini-lung-phantoms with low inter-sample variation that can be scanned simultaneously with the patient undergoing lung quantitative CT.
Keywords: 3D printing; airway measurements; calibration; phantoms; quantitative CT.
© 2021 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals LLC on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
No conflicts of interest.
Figures


References
-
- Chen A, Karwoski RA, Gierada DS, Bartholmai BJ, Koo CW. Quantitative CT analysis of diffuse lung disease. Radiographics. 2020;40:28–43. - PubMed
-
- Goris ML, Zhu HJ, Blankenberg F, Chan F, Robinson TE. An automated approach to quantitative air trapping measurements in mild cystic fibrosis. Chest. 2003;123:1655–1663. - PubMed
-
- Wu X, Kim GH, Salisbury ML, et al, Computed tomographic biomarkers in idiopathic pulmonary fibrosis. The future of quantitative analysis. Am J Respir Crit Care Med. 2019;199:12–21. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
