

Selective vulnerability to atrophy in sporadic Creutzfeldt-Jakob disease
- PMID: 33949799
- PMCID: PMC8164858
- DOI: 10.1002/acn3.51290
Selective vulnerability to atrophy in sporadic Creutzfeldt-Jakob disease
Abstract
Objective: Identification of brain regions susceptible to quantifiable atrophy in sporadic Creutzfeldt-Jakob disease (sCJD) should allow for improved understanding of disease pathophysiology and development of structural biomarkers that might be useful in future treatment trials. Although brain atrophy is not usually present by visual assessment of MRIs in sCJD, we assessed whether using voxel-based morphometry (VBM) can detect group-wise brain atrophy in sCJD.
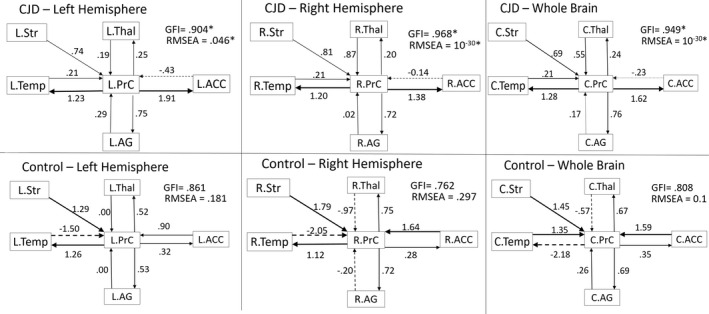
Methods: 3T brain MRI data were analyzed with VBM in 22 sCJD participants and 26 age-matched controls. Analyses included relationships of regional brain volumes with major clinical variables and dichotomization of the cohort according to expected disease duration based on prion molecular classification (i.e., short-duration/Fast-progressors (MM1, MV1, and VV2) vs. long-duration/Slow-progressors (MV2, VV1, and MM2)). Structural equation modeling (SEM) was used to assess network-level interactions of atrophy between specific brain regions.
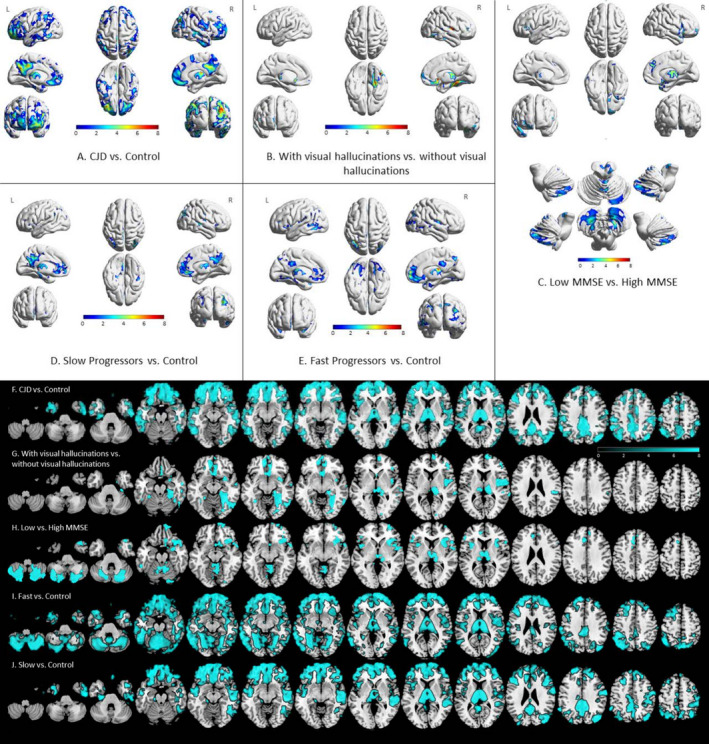
Results: sCJD showed selective atrophy in cortical and subcortical regions overlapping with all but one region of the default mode network (DMN) and the insulae, thalami, and right occipital lobe. SEM showed that the effective connectivity model fit in sCJD but not controls. The presence of visual hallucinations correlated with right fusiform, bilateral thalami, and medial orbitofrontal atrophy. Interestingly, brain atrophy was present in both Fast- and Slow-progressors. Worse cognition was associated with bilateral mesial frontal, insular, temporal pole, thalamus, and cerebellum atrophy.
Interpretation: Brain atrophy in sCJD preferentially affects specific cortical and subcortical regions, with an effective connectivity model showing strength and directionality between regions. Brain atrophy is present in Fast- and Slow-progressors, correlates with clinical findings, and is a potential biomarker in sCJD.
© 2021 The Authors. Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
MDG receives/received research support on prion disease from the NIH/NIA (R01‐AG031189; R56‐AG055619; R01AG062562), the Michael J. Homer Family Fund and Alliance Biosecure. He has consulted for Adept Field Consulting (Backbay consulting), Advanced Medical Inc., Anderson Boutwell Traylor, Acsel Health LLC, Best Doctors Inc., Blade Therapeutics, Biohaven Pharmaceuticals, Bioscience Pharma Partners, LLC (BPP), ClearView HealthCare Partners, Grand Rounds Inc./Second Opinion Inc., Gerson Lehrman Group (GLG) Inc., Guidepoint Global LLC, Market Plus, InThought Consulting, LifeSci Capital LLC, Maupin Cox Legoy, MEDACorp, Quest Diagnostics, 3M Communications (Microvention Terumo), Smith & Hennessey LLC, TeleDoc Health Inc., and Trinity Partners LLC. He has received speaking honoraria for various medical center lectures and from Oakstone Publishing. He has received past research support from CurePSP, the Tau Consortium, Quest Diagnostics, and NIH. Dr. Geschwind serves on the board of directors for San Francisco Bay Area Physicians for Social Responsibility and on the editorial board of
Figures
References
-
- Parchi P, Giese A, Capellari S, et al. Classification of sporadic Creutzfeldt‐Jakob disease based on molecular and phenotypic analysis of 300 subjects. Ann Neurol 1999;46(2):224–233. https://www.ncbi.nlm.nih.gov/pubmed/10443888. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
