

Obesity cardiomyopathy: evidence, mechanisms, and therapeutic implications
- PMID: 33949876
- PMCID: PMC8422427
- DOI: 10.1152/physrev.00030.2020
Obesity cardiomyopathy: evidence, mechanisms, and therapeutic implications
Abstract
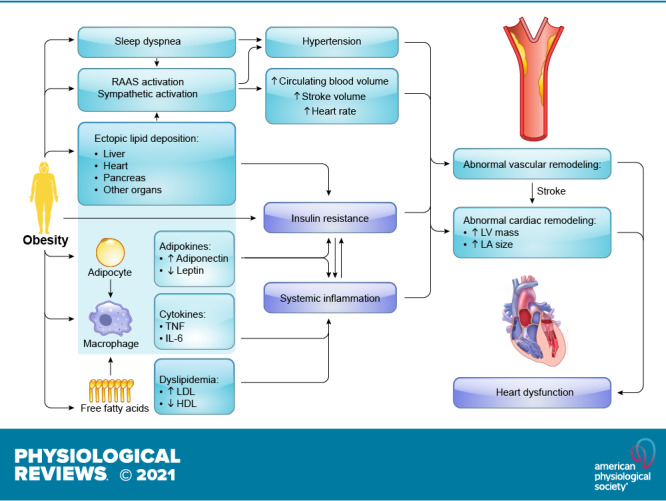
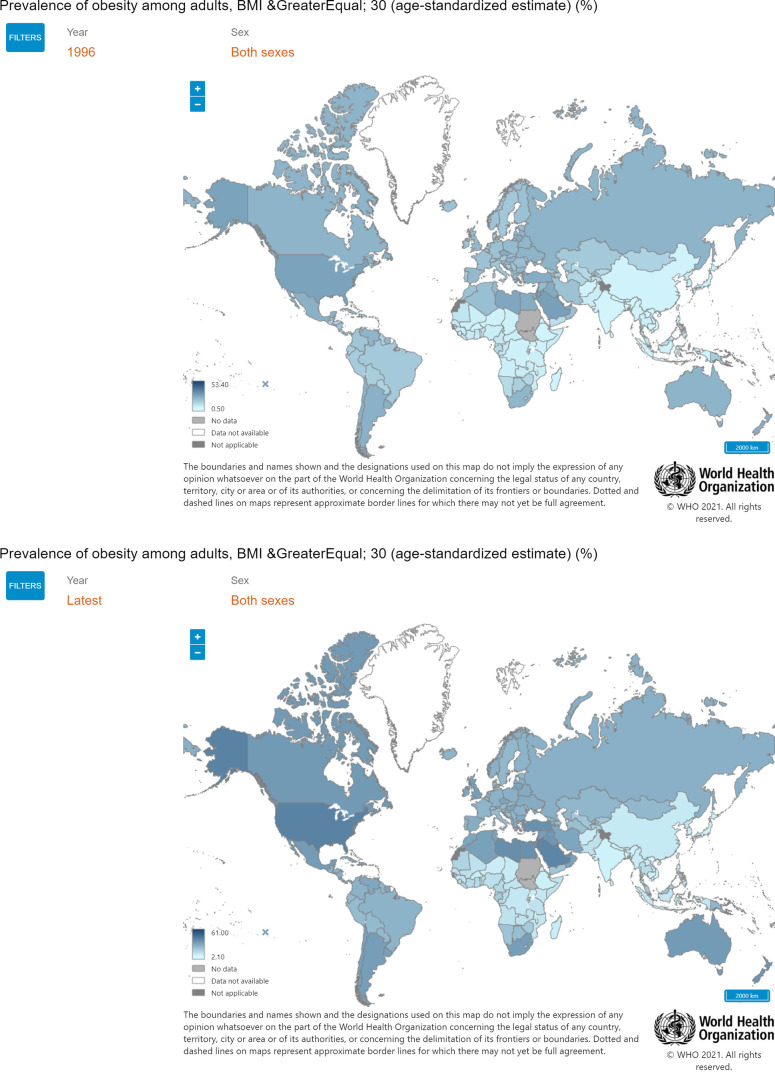
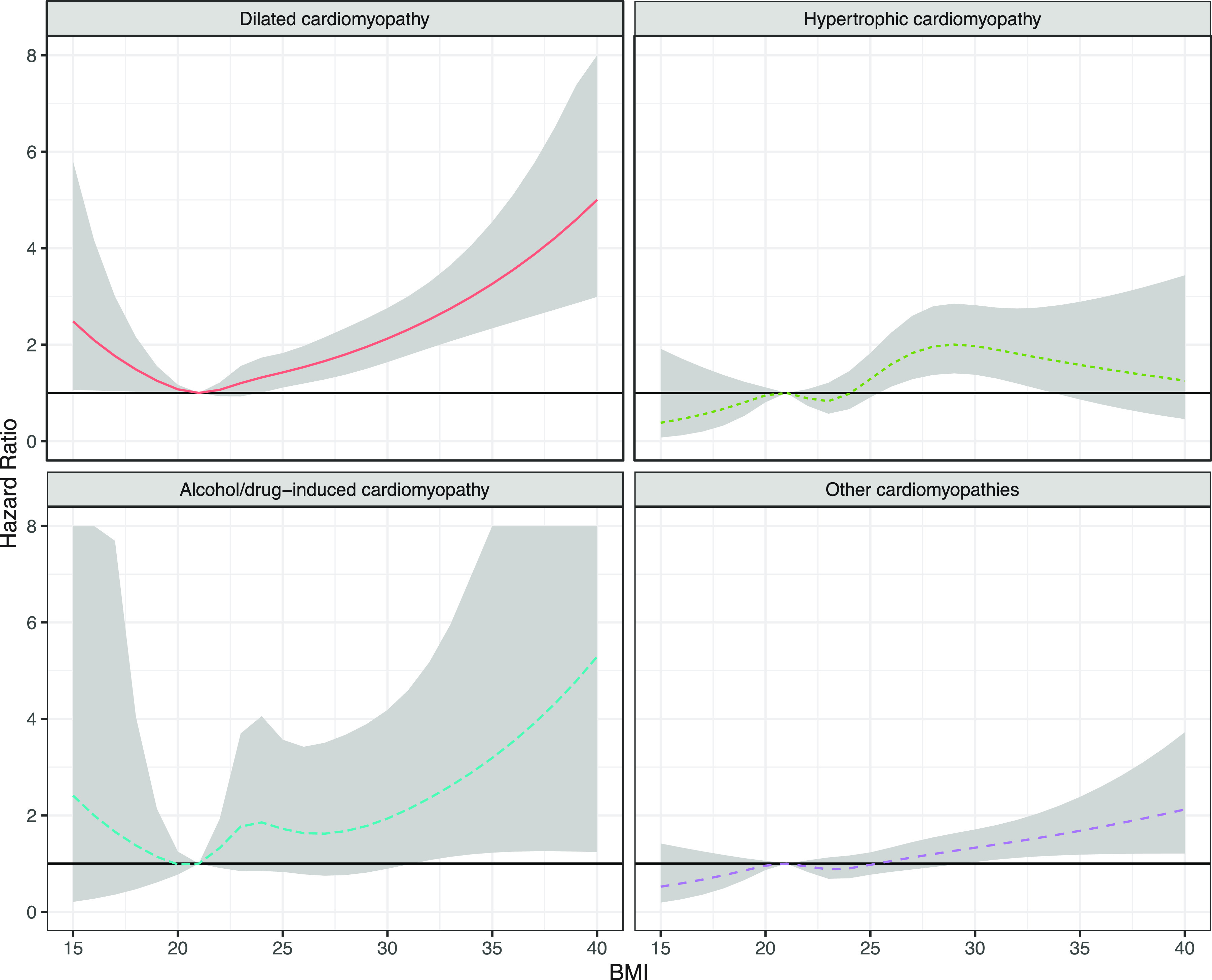
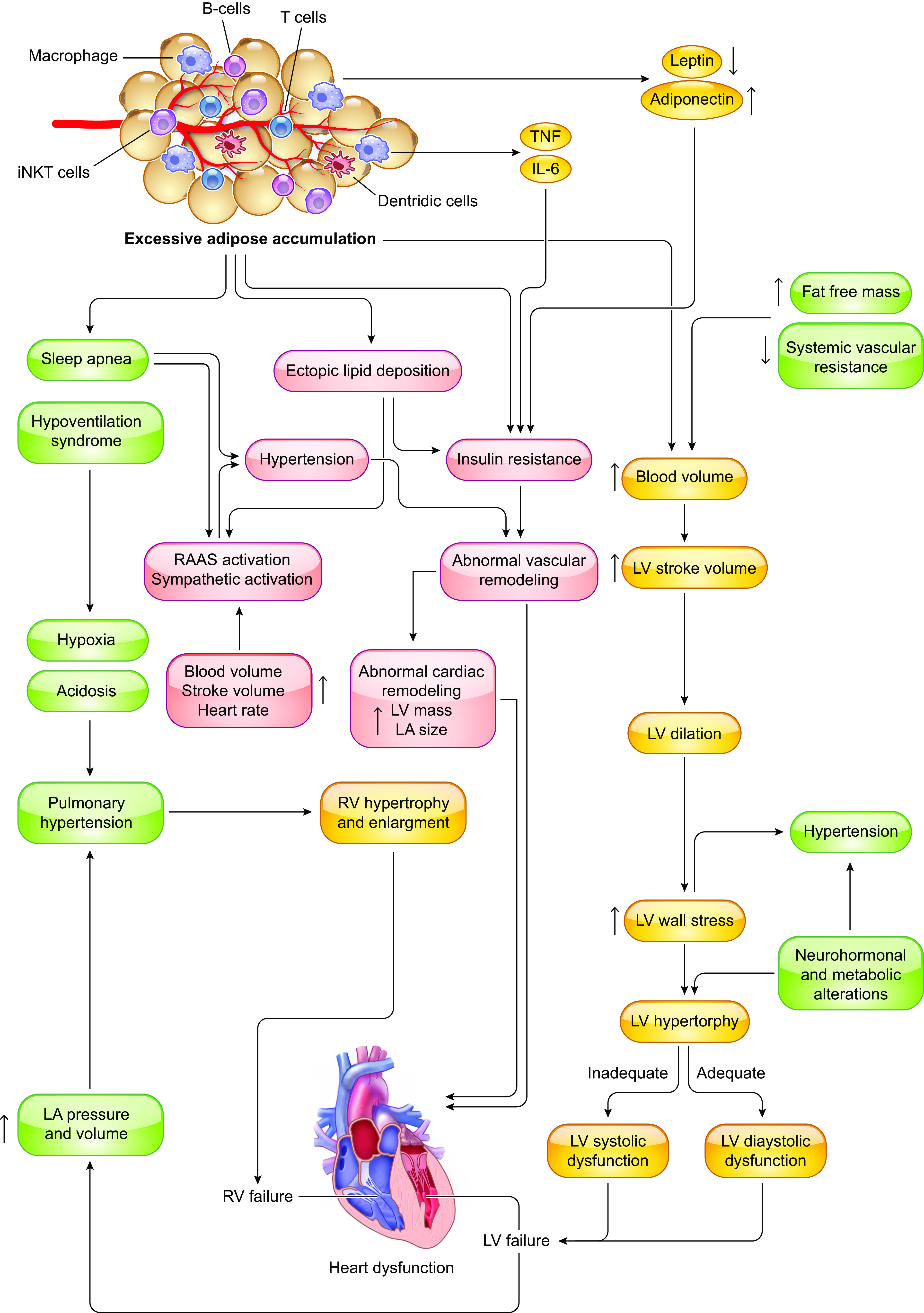
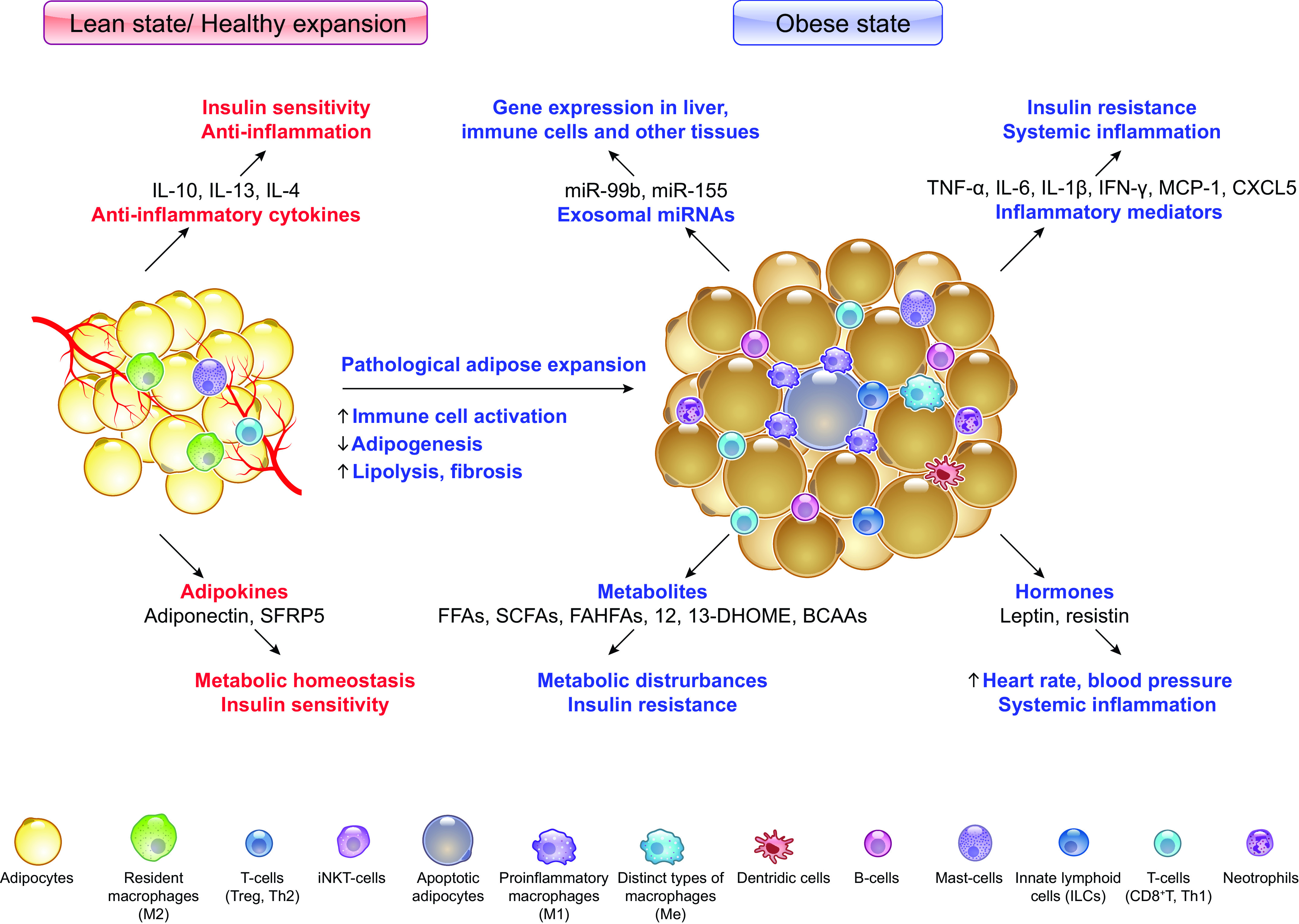
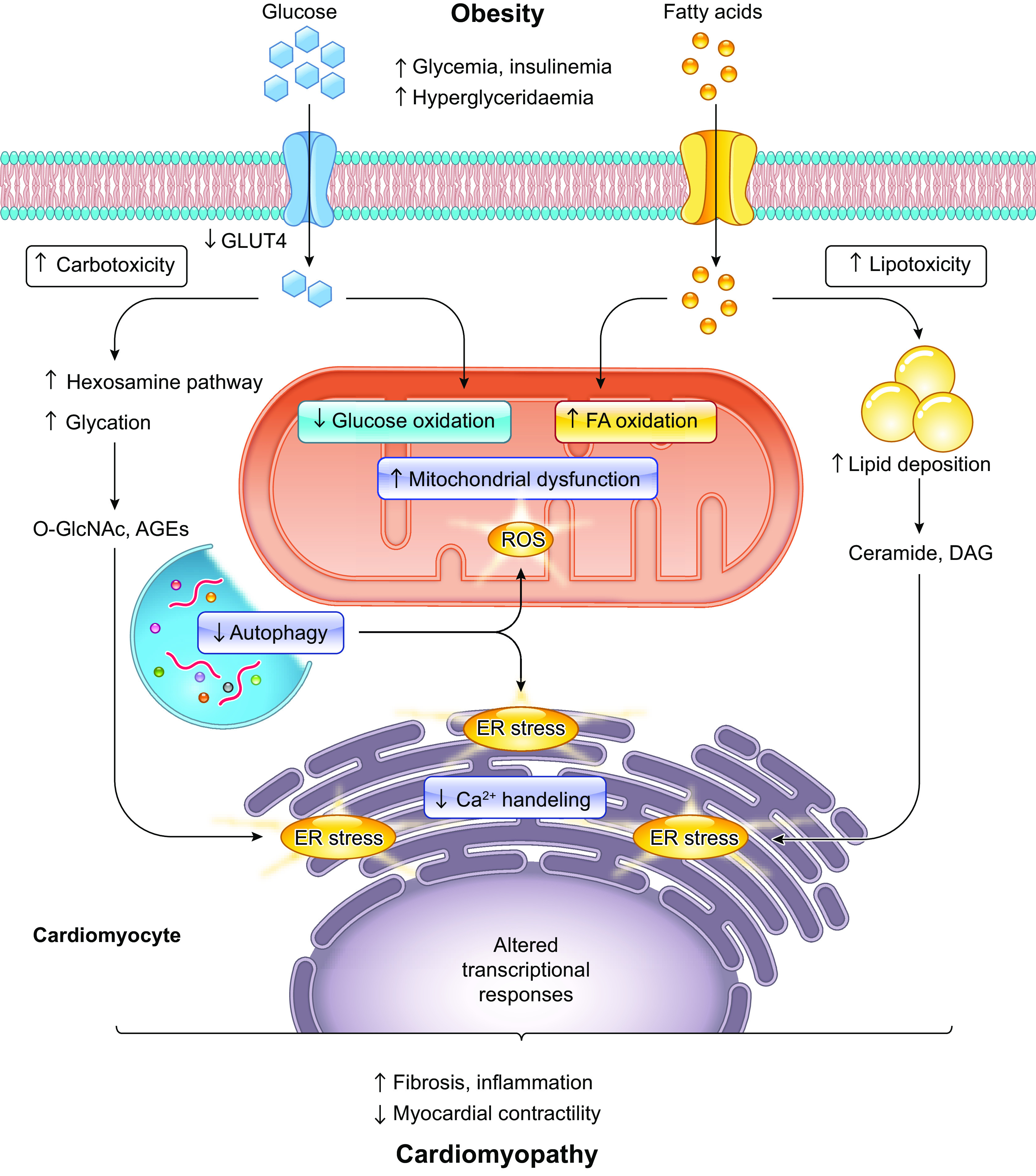
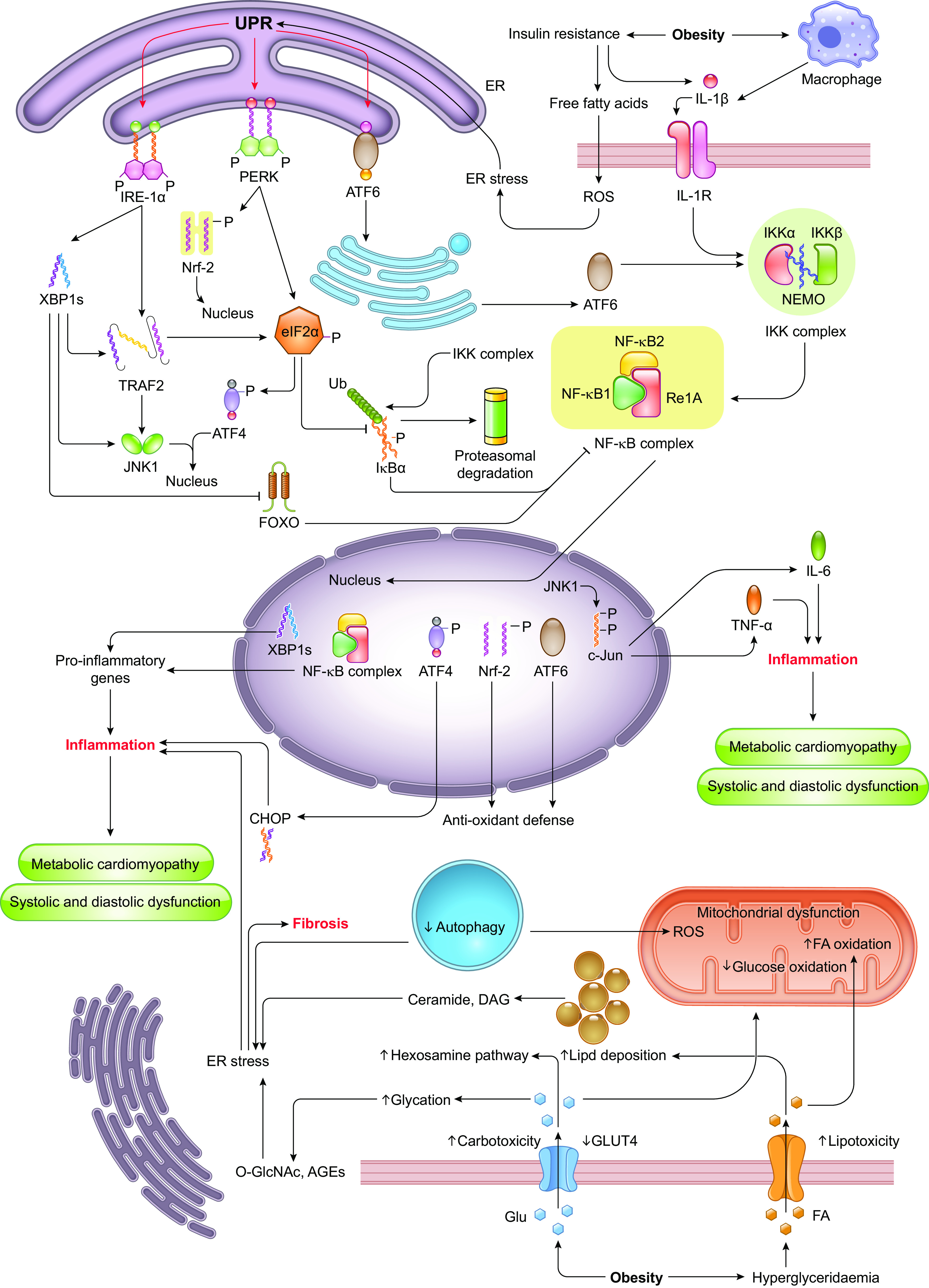
The prevalence of heart failure is on the rise and imposes a major health threat, in part, due to the rapidly increased prevalence of overweight and obesity. To this point, epidemiological, clinical, and experimental evidence supports the existence of a unique disease entity termed "obesity cardiomyopathy," which develops independent of hypertension, coronary heart disease, and other heart diseases. Our contemporary review evaluates the evidence for this pathological condition, examines putative responsible mechanisms, and discusses therapeutic options for this disorder. Clinical findings have consolidated the presence of left ventricular dysfunction in obesity. Experimental investigations have uncovered pathophysiological changes in myocardial structure and function in genetically predisposed and diet-induced obesity. Indeed, contemporary evidence consolidates a wide array of cellular and molecular mechanisms underlying the etiology of obesity cardiomyopathy including adipose tissue dysfunction, systemic inflammation, metabolic disturbances (insulin resistance, abnormal glucose transport, spillover of free fatty acids, lipotoxicity, and amino acid derangement), altered intracellular especially mitochondrial Ca2+ homeostasis, oxidative stress, autophagy/mitophagy defect, myocardial fibrosis, dampened coronary flow reserve, coronary microvascular disease (microangiopathy), and endothelial impairment. Given the important role of obesity in the increased risk of heart failure, especially that with preserved systolic function and the recent rises in COVID-19-associated cardiovascular mortality, this review should provide compelling evidence for the presence of obesity cardiomyopathy, independent of various comorbid conditions, underlying mechanisms, and offer new insights into potential therapeutic approaches (pharmacological and lifestyle modification) for the clinical management of obesity cardiomyopathy.
Keywords: cardiovascular disease; glucotoxicity; heart; inflammation; lipotoxicity; obesity; therapy.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
References
-
- Abarca-Gómez L, Abdeen ZA, Hamid ZA, Abu-Rmeileh NM, Acosta-Cazares B, Acuin C, et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 390: 2627–2642, 2017. doi: 10.1016/S0140-6736(17)32129-3. - DOI - PMC - PubMed
-
- Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 384: 766–781, 2014. doi: 10.1016/S0140-6736(14)60460-8. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous