

Components of clean delivery kits and newborn mortality in the Zambia Chlorhexidine Application Trial (ZamCAT): An observational study
- PMID: 33951036
- PMCID: PMC8133479
- DOI: 10.1371/journal.pmed.1003610
Components of clean delivery kits and newborn mortality in the Zambia Chlorhexidine Application Trial (ZamCAT): An observational study
Abstract
Background: Neonatal infection, a leading cause of neonatal death in low- and middle-income countries, is often caused by pathogens acquired during childbirth. Clean delivery kits (CDKs) have shown efficacy in reducing infection-related perinatal and neonatal mortality. However, there remain gaps in our current knowledge, including the effect of individual components, the timeline of protection, and the benefit of CDKs in home and facility deliveries.
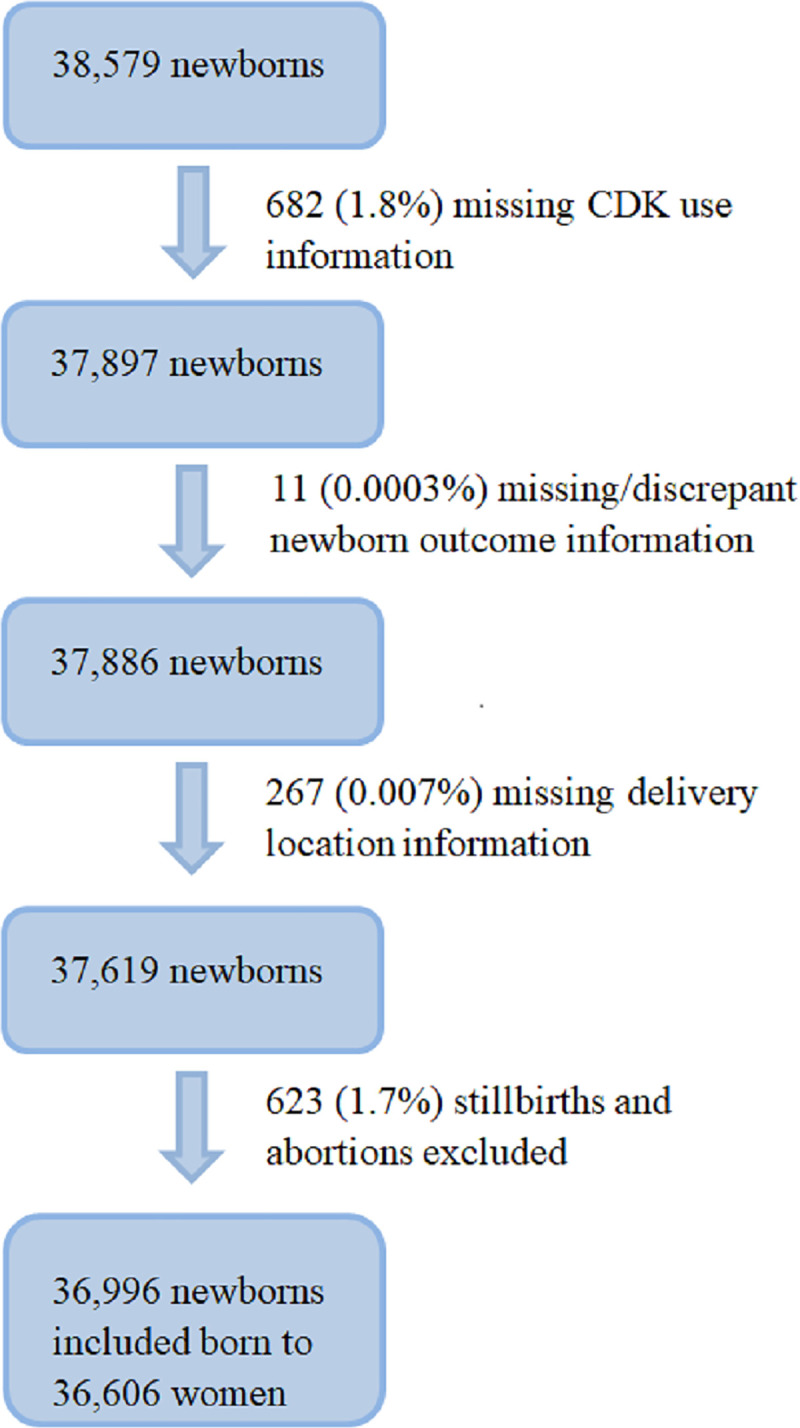
Methods and findings: A post hoc secondary analysis was performed using nonrandomized data from the Zambia Chlorhexidine Application Trial (ZamCAT), a community-based, cluster-randomized controlled trial of chlorhexidine umbilical cord care in Southern Province of Zambia from February 2011 to January 2013. CDKs, containing soap, gloves, cord clamps, plastic sheet, razor blade, matches, and candle, were provided to all pregnant women. Field monitors made a home-based visit to each participant 4 days postpartum, during which CDK use and newborn outcomes were ascertained. Logistic regression was used to study the association between different CDK components and neonatal mortality rate (NMR). Of 38,579 deliveries recorded during the study, 36,996 newborns were analyzed after excluding stillbirths and those with missing information. Gloves, cord clamps, and plastic sheets were the most frequently used CDK item combination in both home and facility deliveries. Each of the 7 CDK components was associated with lower NMR in users versus nonusers. Adjusted logistic regression showed that use of gloves (odds ratio [OR] 0.33, 95% CI 0.24-0.46), cord clamp (OR 0.51, 95% CI 0.38-0.68), plastic sheet (OR 0.46, 95% CI 0.34-0.63), and razor blade (OR 0.69, 95% CI 0.53-0.89) were associated with lower risk of newborn mortality. Use of gloves and cord clamp were associated with reduced risk of immediate newborn death (<24 hours). Reduction in risk of early newborn death (1-6 days) was associated with use of gloves, cord clamps, plastic sheets, and razor blades. In examining perinatal mortality (stillbirth plus neonatal death in the first 7 days of life), similar patterns were observed. There was no significant reduction in risk of late newborn mortality (7-28 days) with CDK use. Study limitations included potential recall bias of CDK use and inability to establish causality, as this was a secondary observational study.
Conclusions: CDK use was associated with reductions in early newborn mortality at both home and facility deliveries, especially when certain kit components were used. While causality could not be established in this nonrandomized secondary analysis, given these beneficial associations, scaling up the use of CDKs in rural areas of sub-Saharan Africa may improve neonatal outcomes.
Trial registration: Name of trial: Zambia Chlorhexidine Application Trial (ZamCAT) Name of registry: Clinicaltrials.gov Trial number: NCT01241318.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Effectiveness of 4% chlorhexidine umbilical cord care on neonatal mortality in Southern Province, Zambia (ZamCAT): a cluster-randomised controlled trial.Lancet Glob Health. 2016 Nov;4(11):e827-e836. doi: 10.1016/S2214-109X(16)30215-7. Epub 2016 Sep 29. Lancet Glob Health. 2016. PMID: 27693439 Clinical Trial.
-
Efficacy of chlorhexidine application to umbilical cord on neonatal mortality in Pemba, Tanzania: a community-based randomised controlled trial.Lancet Glob Health. 2016 Nov;4(11):e837-e844. doi: 10.1016/S2214-109X(16)30223-6. Epub 2016 Sep 29. Lancet Glob Health. 2016. PMID: 27693438 Clinical Trial.
-
Influence of newborn health messages on care-seeking practices and community health behaviors among participants in the Zambia Chlorhexidine Application Trial.PLoS One. 2018 Jun 14;13(6):e0198176. doi: 10.1371/journal.pone.0198176. eCollection 2018. PLoS One. 2018. PMID: 29902234 Free PMC article. Clinical Trial.
-
Application of 4% chlorhexidine to the umbilical cord stump of newborn infants in lower income countries: a systematic review and meta-analysis.Matern Health Neonatol Perinatol. 2019 Oct 17;5:16. doi: 10.1186/s40748-019-0111-y. eCollection 2019. Matern Health Neonatol Perinatol. 2019. Retraction in: Matern Health Neonatol Perinatol. 2020 Jun 16;6:4. doi: 10.1186/s40748-020-00118-y. PMID: 31641528 Free PMC article. Retracted. Review.
-
Safety and impact of chlorhexidine antisepsis interventions for improving neonatal health in developing countries.Pediatr Infect Dis J. 2006 Aug;25(8):665-75. doi: 10.1097/01.inf.0000223489.02791.70. Pediatr Infect Dis J. 2006. PMID: 16874163 Free PMC article. Review.
Cited by
-
Can Clean Delivery Kits Prevent Infections? Lessons from Traditional Birth Attendants in Nigeria.Ann Glob Health. 2023 Dec 6;89(1):85. doi: 10.5334/aogh.4015. eCollection 2023. Ann Glob Health. 2023. PMID: 38077261 Free PMC article. Clinical Trial.
-
Effect of perinatal sterile gloves on neonatal mortality: a post hoc analysis of a randomised clinical trial in Zambia.Transl Pediatr. 2025 Jul 31;14(7):1422-1431. doi: 10.21037/tp-2025-88. Epub 2025 Jul 28. Transl Pediatr. 2025. PMID: 40800172 Free PMC article.
-
Effect of Maternal and Newborn Care Service Package on Perinatal and Newborn Mortality: A Cluster Randomized Clinical Trial.JAMA Netw Open. 2024 Feb 5;7(2):e2356609. doi: 10.1001/jamanetworkopen.2023.56609. JAMA Netw Open. 2024. PMID: 38372998 Free PMC article. Clinical Trial.
References
-
- Alliance for Maternal and Newborn Health Improvement (AMANHI) mortality study group. Population-based rates, timing, and causes of maternal deaths, stillbirths, and neonatal deaths in south Asia and sub-Saharan Africa: a multi-country prospective cohort study. Lancet Glob Health. 2018;6(12):e1297–308. 10.1016/S2214-109X(18)30385-1 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
