

Four-Month Rifapentine Regimens with or without Moxifloxacin for Tuberculosis
- PMID: 33951360
- PMCID: PMC8282329
- DOI: 10.1056/NEJMoa2033400
Four-Month Rifapentine Regimens with or without Moxifloxacin for Tuberculosis
Abstract
Background: Rifapentine-based regimens have potent antimycobacterial activity that may allow for a shorter course in patients with drug-susceptible pulmonary tuberculosis.
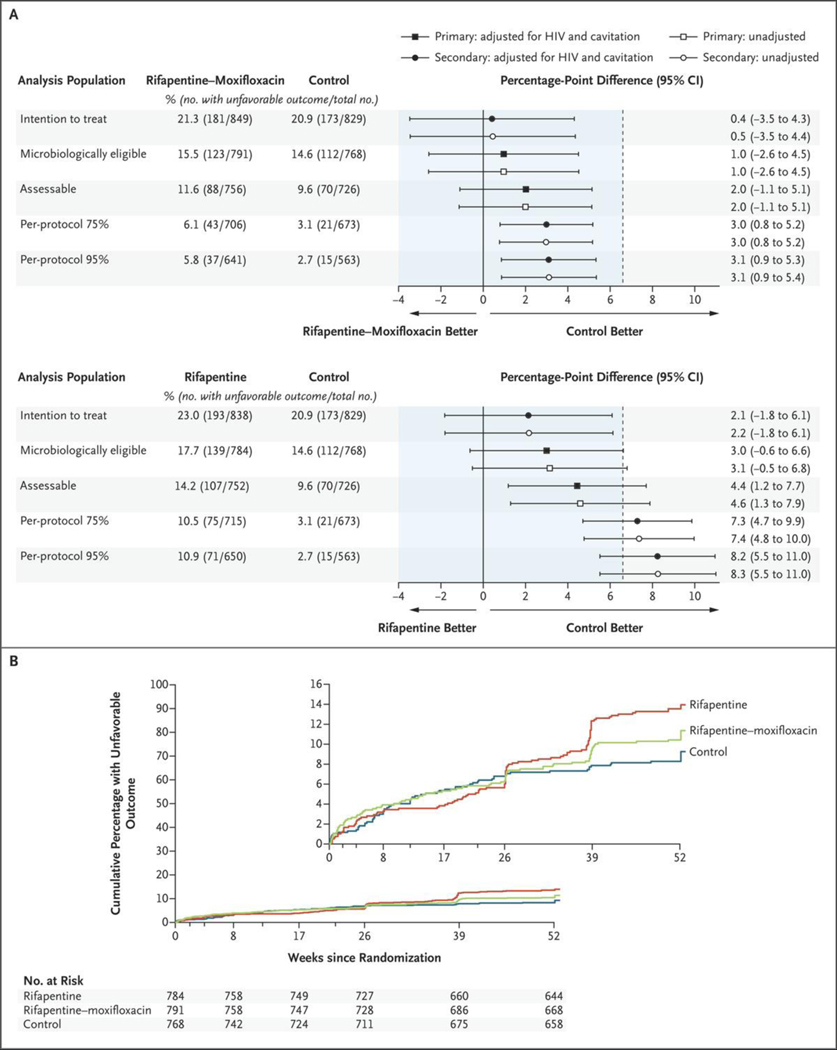
Methods: In an open-label, phase 3, randomized, controlled trial involving persons with newly diagnosed pulmonary tuberculosis from 13 countries, we compared two 4-month rifapentine-based regimens with a standard 6-month regimen consisting of rifampin, isoniazid, pyrazinamide, and ethambutol (control) using a noninferiority margin of 6.6 percentage points. In one 4-month regimen, rifampin was replaced with rifapentine; in the other, rifampin was replaced with rifapentine and ethambutol with moxifloxacin. The primary efficacy outcome was survival free of tuberculosis at 12 months.
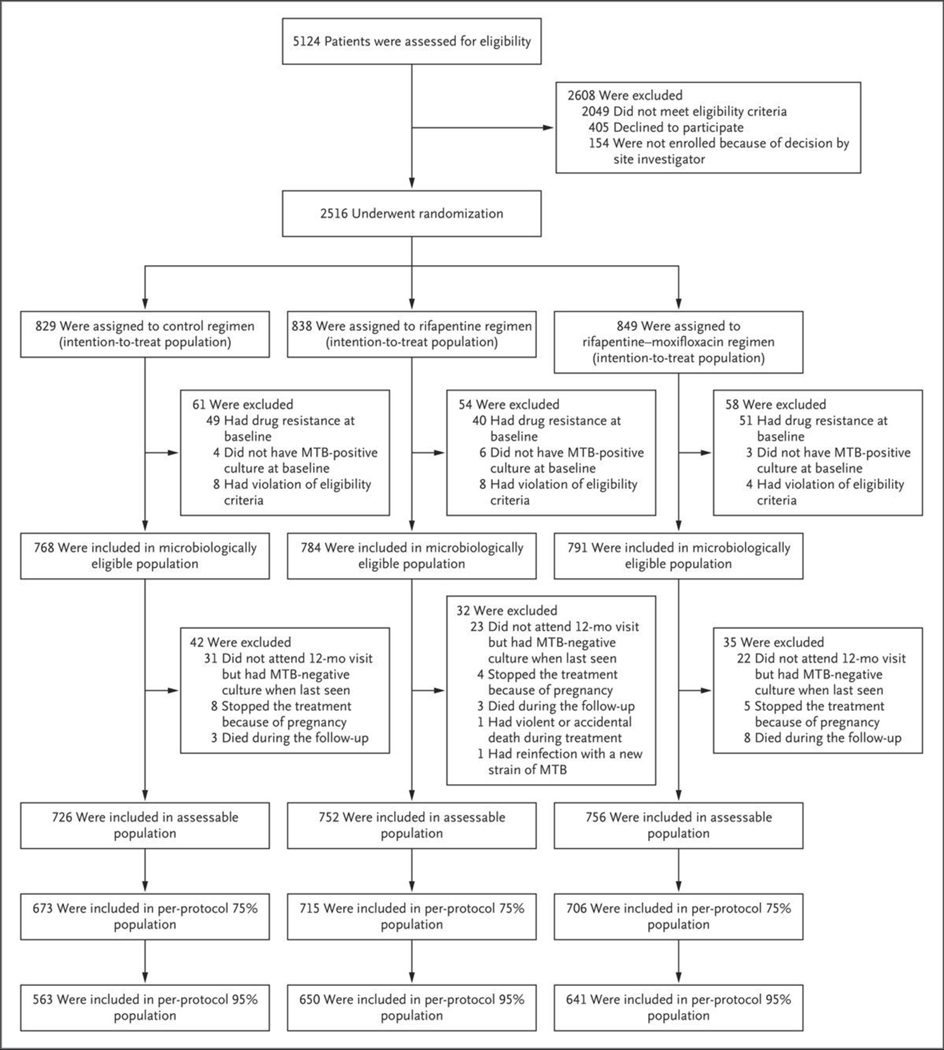
Results: Among 2516 participants who had undergone randomization, 2343 had a culture positive for Mycobacterium tuberculosis that was not resistant to isoniazid, rifampin, or fluoroquinolones (microbiologically eligible population; 768 in the control group, 791 in the rifapentine-moxifloxacin group, and 784 in the rifapentine group), of whom 194 were coinfected with human immunodeficiency virus and 1703 had cavitation on chest radiography. A total of 2234 participants could be assessed for the primary outcome (assessable population; 726 in the control group, 756 in the rifapentine-moxifloxacin group, and 752 in the rifapentine group). Rifapentine with moxifloxacin was noninferior to the control in the microbiologically eligible population (15.5% vs. 14.6% had an unfavorable outcome; difference, 1.0 percentage point; 95% confidence interval [CI], -2.6 to 4.5) and in the assessable population (11.6% vs. 9.6%; difference, 2.0 percentage points; 95% CI, -1.1 to 5.1). Noninferiority was shown in the secondary and sensitivity analyses. Rifapentine without moxifloxacin was not shown to be noninferior to the control in either population (17.7% vs. 14.6% with an unfavorable outcome in the microbiologically eligible population; difference, 3.0 percentage points [95% CI, -0.6 to 6.6]; and 14.2% vs. 9.6% in the assessable population; difference, 4.4 percentage points [95% CI, 1.2 to 7.7]). Adverse events of grade 3 or higher occurred during the on-treatment period in 19.3% of participants in the control group, 18.8% in the rifapentine-moxifloxacin group, and 14.3% in the rifapentine group.
Conclusions: The efficacy of a 4-month rifapentine-based regimen containing moxifloxacin was noninferior to the standard 6-month regimen in the treatment of tuberculosis. (Funded by the Centers for Disease Control and Prevention and others; Study 31/A5349 ClinicalTrials.gov number, NCT02410772.).
Copyright © 2021 Massachusetts Medical Society.
Figures
Comment in
-
Shortening the Short Course of Tuberculosis Treatment.N Engl J Med. 2021 May 6;384(18):1764-1765. doi: 10.1056/NEJMe2104499. N Engl J Med. 2021. PMID: 33951367 No abstract available.
-
Four-Month Rifapentine Regimens for Tuberculosis.N Engl J Med. 2022 Mar 17;386(11):1095. doi: 10.1056/NEJMc2114483. N Engl J Med. 2022. PMID: 35294822 No abstract available.
References
-
- Guidelines for treatment of drug-susceptible tuberculosis and patient care, 2017 update. Geneva: World Health Organization, April 2017. (https://www.who.int/tb/publications/2017/dstb_guidance_2017/en/).
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical